Strategic Plan Adopted by the National Registry Board
The National Registry Board of Directors adopted its first formal strategic plan to guide the development of national EMS certification. This effort marked a shift toward long-term organizational planning and evidence-based leadership. The LEADS committee completed its second national EMS workforce survey, laying the groundwork for future data-driven decisions.
 Source:
Source: 




 Source:
Source: 


 Image: EMS Compass Project – NASEMSO/NHTSA
Image: EMS Compass Project – NASEMSO/NHTSA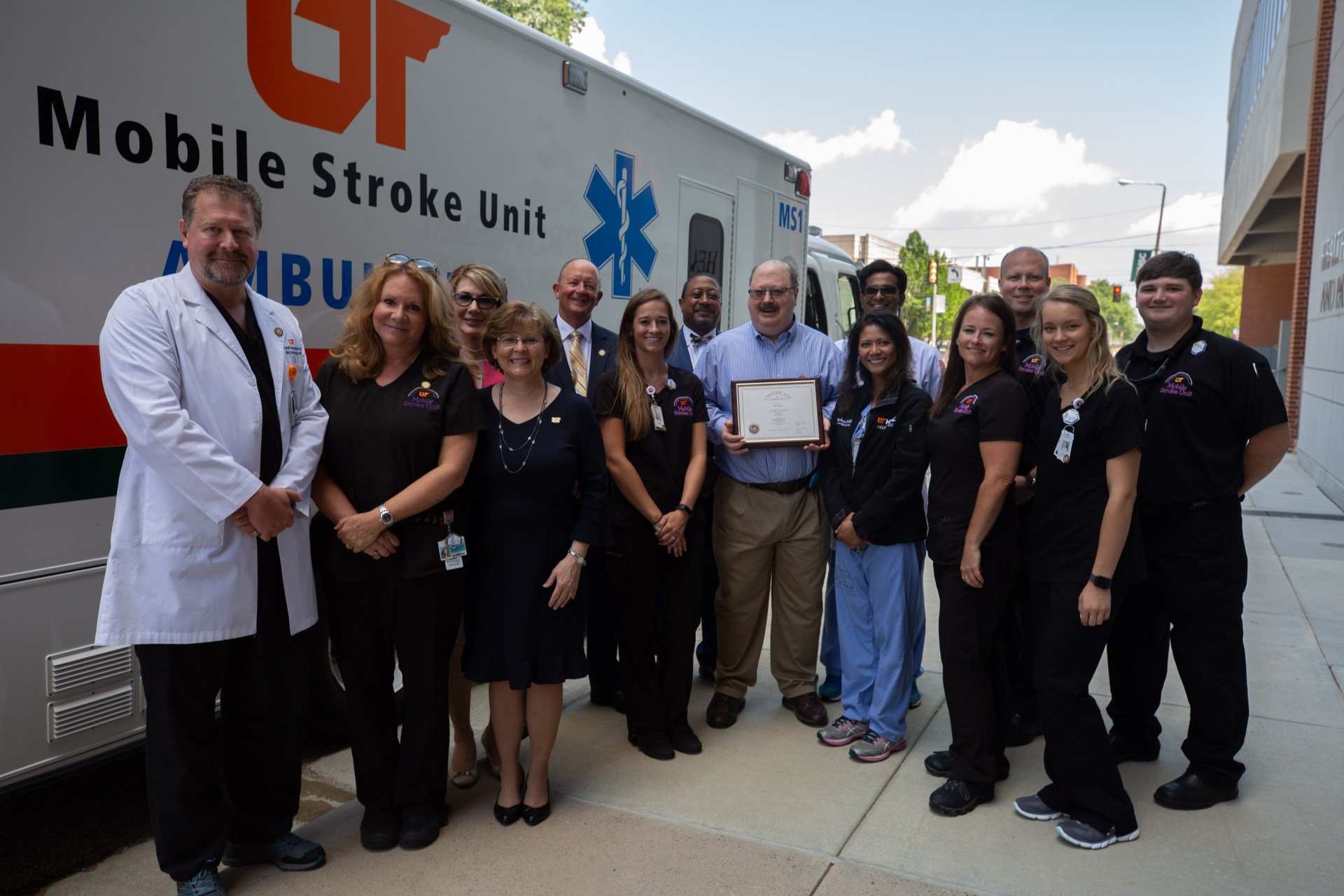


 October 7, 2017 — The inaugural Commissioners for the first meeting of the Interstate Commission for EMS Personnel Practice. Front (L–R): Jeanne-Marie Bakehouse (CO), Donna G. Tidwell (TN), Alisa Williams (MS), Joe Schmider (TX). Back Row (L–R): Wayne Denny (ID), Guy Dansie (UT), Diane McGinnis Hainsworth (DE), Stephen Wilson (AL), Andy Gienapp (WY), Joe House (KS), Gary Brown (VA). Not pictured: Keith Wages (GA).
October 7, 2017 — The inaugural Commissioners for the first meeting of the Interstate Commission for EMS Personnel Practice. Front (L–R): Jeanne-Marie Bakehouse (CO), Donna G. Tidwell (TN), Alisa Williams (MS), Joe Schmider (TX). Back Row (L–R): Wayne Denny (ID), Guy Dansie (UT), Diane McGinnis Hainsworth (DE), Stephen Wilson (AL), Andy Gienapp (WY), Joe House (KS), Gary Brown (VA). Not pictured: Keith Wages (GA).