The Dark Ages
of EMS
How America Created, then Forgot, Its Early Emergency Medical Legacy
About This Book
Why does EMS have the issues it faces today? The Dark Ages of EMS answers that question through historical perspectives, connecting the defunding decisions of the 1980s to the systemic challenges that persist in modern emergency medical services.
Most histories of EMS begin in 1966, with the publication of the White Paper. The conventional narrative holds that organized emergency medical services essentially did not exist before that moment. The Dark Ages of EMS demonstrates that American cities had built sophisticated, physician-staffed, hospital-integrated ambulance systems by the 1880s — and that the century of development that preceded 1966, including what was built, what was destroyed, and what was incompletely rebuilt, is not background. It is the explanation.
This book traces that arc: from the illumination of the pre-war era, through the dark age of the mid-twentieth century, into the incomplete renaissance that followed, and into the present, where the profession confronts not only the external forces that have always constrained it but the internal resistance that now compounds them.
Who Should Read This Book
What's Inside
10 chapters tracing the arc of American EMS
Every chapter of The Dark Ages of EMS is available here — listen or read online, completely free. No signup, no paywall. This is our gift to the EMS community.
Want the paperback or hardcover? Buy on Amazon. Prefer to read offline? Download the free EPUB.
The crisis of the American
emergency medical services system
is not that the profession is young.
It is that the profession is old,
and it was rebuilt on the ruins of something
it no longer remembers.
In 1889, a Chicago police officer climbed into the back of a horse-drawn ambulance carrying tourniquets, splints, wound disinfectant, and an emetic protocol for poisoning cases. He had been trained to control hemorrhage, assess trauma patients, and apply structured clinical interventions by protocol. He was dispatched to emergencies through an integrated municipal system, funded by the city, and backed by the institutional authority of a major metropolitan government.
Today, state legislatures across the country are contemplating legislation lowering training standards, distancing EMS from the medical professions it was built to join, and drafting bills to let individuals trained in just CPR or basic first aid, staff ambulances. The systems that were supposed to provide emergency medical care have run out of people to send.
The distance between those two sentences is the subject of this book.
Most histories of emergency medical services in the United States begin in 1966, with the publication of Accidental Death and Disability: The Neglected Disease of Modern Society, the landmark National Academy of Sciences report known simply as the White Paper. The conventional narrative holds that organized emergency medical services essentially did not exist before that document sounded the alarm, and that everything recognizable as modern EMS was built in the decade that followed. It is a tidy origin story. It is also incomplete.
The reality is that American cities had built sophisticated, physician-staffed, hospital-integrated ambulance systems by the 1880s. These were not primitive forerunners of the real thing. They were funded municipal services with trained medical professionals, purpose-built vehicles, communications infrastructure, and clinical missions that would be recognizable to any EMS leader working today. That infrastructure expanded for half a century. Then the Great Depression hollowed it out, two world wars stripped it of personnel, and the funeral industry filled the vacuum with hearses driven by mortuary attendants who had never taken a first aid course. By the time the White Paper authors surveyed the wreckage in 1966, the earlier systems had been forgotten so thoroughly that the report read as a discovery of something new rather than a recognition of something lost.
The rebuilders of the 1960s and 1970s were genuine visionaries. They created the modern paramedic, a clinical role without historical precedent, and they saved countless lives in the process. But they built their new profession on a set of compromises that were supposed to be temporary: minimal training thresholds that were meant to be floors, not ceilings; a reimbursement structure that paid for transport rather than clinical care; a patchwork of fifty separate state regulatory systems with no unifying federal architecture. The nation was supposed to come back and finish the work. It never did.
This book traces that arc: from the illumination of the pre-war era, through the dark age of the mid-twentieth century, into the incomplete renaissance that followed, and finally into the present, where the profession confronts not only the external forces that have always constrained it but the internal resistance that now compounds them. It is a history, but it is not offered as an academic exercise. It is offered because the structural problems that define American EMS in 2026, the funding crises, the workforce shortages, the credentialing fragmentation, the professional marginalization, are not new problems. They are old problems, rooted in a collapse that happened nearly a century ago and a rebuilding that was never completed. Understanding where those problems came from is a prerequisite to solving them.
The framework for this book came not from an EMS conference or a policy paper, but from standing in the ruins of Rome and Corinth — cities that built aqueducts, surgical instruments, and public health infrastructure not matched for a thousand years after their collapse. The parallel to American EMS was not subtle. It was exact.
A word about tone. Some chapters of this book, "The Broken Promise" and "The Enemy Within," will make some readers uncomfortable. It is intended to. The chapters examine documented instances in which segments of the EMS profession itself have resisted the reforms necessary for its own advancement: opposing portable credentials, exempting practitioners from accountability standards applied to every other healthcare discipline, blocking educational requirements that comparable professions adopted decades ago. These are not accusations leveled from the outside. They are observations made by someone who has spent a career inside this profession, who cares deeply about its future, and who believes that intellectual honesty requires naming the problem even when the problem is us. The argument is not that every institutional actor within EMS is obstructing progress. It is that enough of them are, on enough fronts, that the pattern can no longer be ignored.
I wrote this book because I believe the EMS profession deserves to know its own history, including the parts that have been forgotten and the parts that are difficult to confront. The paramedics, EMTs, and emergency medical dispatchers who answer the call every day deserve a profession with the institutional standing, the financial architecture, and the political recognition that their work has always warranted. Building that profession requires understanding why it does not yet exist. That understanding begins here.
A note on the timeline. The conventional narrative places the origin of American EMS in 1966, with the publication of the White Paper. This book demonstrates that the history of organized ambulance medicine in the United States stretches back more than a hundred and sixty years—and that the century of development that preceded 1966, including what was built, what was destroyed, and what was incompletely rebuilt, is not background. It is the explanation. The structural crises that define EMS in 2026 cannot be understood without it, and they will not be resolved by a profession that does not know it happened.
— Donnie Woodyard, Jr.
Chapter 1 — Is EMS Essential?
On February 2, 2026, the South Dakota Senate Health and Human Services Committee stripped the word essential from a bill that would have required cities and counties to guarantee access to emergency medical services. The bill’s own sponsor, Senator Tim Reed, asked for the removal.1
“We’re not ready to designate emergency medical services as essential — yet,” Reed said.1
The reason was not philosophical; it was financial. As Brian Hambek, president of the South Dakota Ambulance Association, told the committee: “Listing us as an essential service without funding to back it is useless.”1 The state had gone from 131 ambulance services to 121 in the last decade, and most of South Dakota’s EMTs were volunteers with an average age of 52.2 Ambulance transport billing and reimbursements did not cover costs, and among the legislature’s proposed remedies to this crisis was a bill to let police officers drive ambulances and another to lower the training threshold for emergency response.1
This is 2026 in the United States, not 1956, and not in a developing nation. Consider the details: aging volunteers, untrained drivers, services disappearing from rural communities, and lawmakers unwilling to fund what everyone acknowledges is necessary. Tragically, South Dakota is not an outlier. It is a mirror.
To be clear, the underlying logic of Senator Reed’s revised position is sound. Designating EMS as “essential” without a funding source is an unfunded mandate—a label without architecture. But that is precisely the point. The absence of financial architecture for emergency medical services is not a new failure. It is the foundational compromise of the post-World War II era, still unresolved.
To understand why a state legislature in 2026 cannot bring itself to call ambulance service essential and fund it, you have to go further back in history than most people expect.
To understand why a state legislature in 2026 cannot bring itself to call ambulance service essential and fund it, you must go further back in history than most people expect.
“We’re not ready to designate emergency medical services as essential — yet,”
Hult, J. (2026, February 2). South Dakota lawmakers not ready to call emergency medical services essential. South Dakota Searchlight.
Chapter 2 — The Illumination (1860s–1930s)
Before the world wars, American cities had built sophisticated, physician-staffed, purpose-designed ambulance systems. This was not proto-EMS or some quaint antecedent to the real thing. It was an advanced, funded, and functioning emergency medical infrastructure built on an assumption that has since been abandoned: that the medical professionals who arrive on an ambulance should be among the most qualified clinicians available in a city.
The story begins, as so many stories in emergency medicine do, on a battlefield. The American Civil War produced the first organized ambulance corps, and its innovations transferred to civilian medicine with remarkable speed. In 1861, the United States Sanitary Commission established the organizational framework for coordinated emergency response.3 The following year, Jonathan Letterman, Medical Director of the Army of the Potomac, created his legendary ambulance corps: a system of triage, forward aid stations, and structured evacuation that transformed the chaos of battlefield medicine into something approaching a rational architecture of care.4

Ambulance Corps teams demonstrate battlefield evacuation techniques during the American Civil War, carefully removing wounded soldiers from the field for transport to field hospitals (photograph by William Frank Browne, c. 1861–1869).
The military-to-civilian pipeline was rapid and intentional. By 1865, only three years after Letterman’s reforms, Cincinnati’s Commercial Hospital had launched the first civilian ambulance service in the United States. Municipal employment records document James R. Jackson as a paid ambulance driver as early as that year—the first known salaried civilian ambulance professional in American history.5 Four years after that, in 1869, Bellevue Hospital in New York City established what is now widely recognized as the first comprehensive hospital-based ambulance service in the world.6,7 Bellevue’s ambulances carried physicians. They carried surgical kits. They were dispatched by telegraph, and they were fully integrated into the hospital’s emergency response system.

Bellevue Hospital, 1885.
What followed was an era of genuine civic competition. By the late nineteenth and early twentieth century, major American cities were not merely maintaining ambulance services, but they were competing and racing to build better ones. The ambulance service was a matter of public expectation and civic prestige. In 1871, a traveler’s guide to New York City featured the Bellevue ambulance system as a point of urban pride, something visitors should know about, like Central Park or the Brooklyn Bridge. The following year, ambulance operations had become so routine that they generated the profession’s first legal liability: in 1872, a pedestrian struck by a horse-drawn ambulance in New York brought what appears to be the earliest ambulance-related court case in American history—a small detail, but one that speaks to how deeply embedded these services had become in the fabric of urban life.
St. Louis launched its ambulance service in 1875. That same year, Hugh Owen Thomas invented the Thomas Splint. This device would later reduce femur fracture mortality from roughly 80% to under 16% when widely deployed in World War I—a reduction driven by the splint alongside improved evacuation and wound care—and a reminder that the era’s innovations were not limited to vehicle design and dispatch systems but extended to the clinical tools carried aboard the ambulances themselves. Other cities followed rapidly. In 1884, Bellevue graduated its first formal class of ambulance surgeons. The ambulance surgeon position was a competitive, prestigious medical appointment that attracted top graduates.9 In 1895, the New York City Police Department deployed a bicycle ambulance corps to improve response times in congested neighborhoods. In 1899, Michael Reese Hospital in Chicago placed the first automobile-powered ambulance in service. By 1903, Dr. Emily Dunning Barringer had become the first female ambulance surgeon at Gouverneur Hospital in New York.10 The title itself—ambulance surgeon—tells you everything about the clinical expectations of the era.
The clinical seriousness of these early systems is perhaps best illustrated at the street level. In 1889, Chicago’s first horse-drawn police ambulance carried tourniquets, splints, wound disinfectant, an emetic protocol for poisoning cases, and environmental medicine supplies for sunstroke—a deliberate clinical loadout, not just a simple first aid kit.34 By 1895, a Chicago Tribune reporter who spent a full day embedded with the city’s ambulance crews documented officers performing tourniquet application for traumatic amputations, hemorrhage control, and structured patient assessment—clinical interventions delivered by protocol, in the field, years before the twentieth century began.34
The spirit of innovation extended to vehicle design itself. In 1896, Dr. J.T. Binkley Jr. built a cycle ambulance for Chicago Hospital. It featured a patient compartment suspended between two tandem bicycles, weighing 148 pounds, capable of seventeen miles per hour, with a glass ventilating window and Red Cross insignia. It was trialed on July 30, 1896, and deployed the very next day for injuries during a bicycle road race. Patients reportedly preferred it to the horse-drawn ambulances.34 The invention was a small episode, but it captured the culture of the era: a physician designing a purpose-built, lightweight patient transport vehicle optimized for speed and comfort, on his own initiative, because he believed the existing system could be improved.
By 1909, Indianapolis, Indiana, was deploying electric ambulances engineered with air-ride suspension for patient comfort, and the Indianapolis Motor Speedway had organized dedicated medical standby coverage for its opening events.11 These innovations were not primitive conveyances, but purpose-built medical vehicles staffed by highly trained and specialized medical professionals. More importantly, they were funded as core parts of a city’s municipal budget, alongside police, fire, schools, and all other essential services associated with a city.
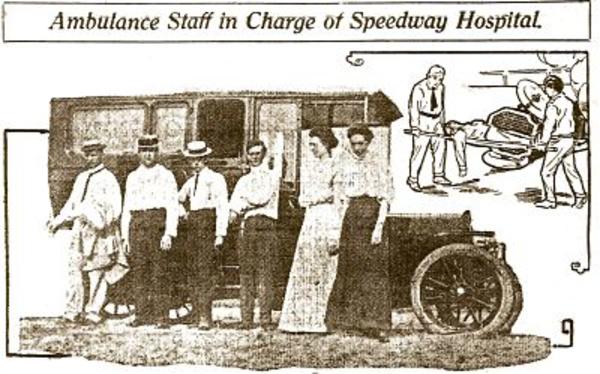
1909, Ambulance at the 1st Indianapolis Motor Speedway race.
A necessary honesty: at this time, the development of prehospital medical care was impressive, but it was overwhelmingly an urban achievement. The physician-staffed ambulances of New York, Chicago, Cincinnati, and Indianapolis served dense city populations with concentrated hospital infrastructure and robust municipal tax bases. Rural America in 1890 had little or nothing; no organized ambulance service, no telegraph dispatch, no physician responding to emergencies in the field. The Illumination, for all its genuine sophistication, never reached the communities that had the least access to medical care and needed it most. That limitation matters, and it would be dishonest to romanticize the era without acknowledging it. But it also sharpens the tragedy of what followed. The urban model was not static. It was expanding—city by city, decade by decade, the infrastructure was being built outward. Brooklyn followed Manhattan. Indianapolis followed Chicago. Smaller cities and towns were learning from the cities and smaller services were beginning to fill the gaps in places too small for municipal systems. The Dark Age of EMS did not merely destroy what existed. It destroyed what was still becoming—and the communities that were next in line for organized emergency medical care were precisely the ones left waiting longest when the collapse came.
The Dark Age of EMS did not merely destroy what existed. It destroyed what was still becoming.
Unfortunately, Chicago's early leadership in out-of-hospital emergency care did not endure. The police ambulances that had carried medical equipment and trained officers in the 1890s gradually lost their clinical character as motorization arrived. By the 1910s, the department had phased out dedicated ambulance wagons in favor of using motorized patrol wagons—the "black marias"—to double as emergency transport, a shift driven by efficiency and budget concerns that effectively ended the police ambulance service as a standalone medical unit. According to the historical records, in 1920, what remained of the service was formally transferred back to the Chicago Police Department (the phrasing "transferred back" suggests it had been reassigned elsewhere during the Progressive Era or World War I), but by then it was a shell of its former self—basic transport, not medical care.
Hospital-based ambulances tried to fill the void. Michael Reese Hospital's 1899 motorized ambulance continued operating into the 1920s, as did Cook County Hospital's "hospital on wheels" launched in 1907. But these were institution-specific assets, serving each hospital's immediate catchment rather than the city as a whole. The rest of the gap was filled by private ambulances—most operated by funeral home directors using their hearses, outfitted with a stretcher, blankets, and a first-aid kit. By the mid-1920s, Chicago's emergency transport had devolved into a fragmented patchwork: police wagons, hospital cars, and undertakers' vehicles, with no centralized oversight and no consistent medical staffing.
The Chicago Fire Department's 1928 entry into ambulance service was a response to this recognized void. On November 1, 1928, the CFD placed six motorized ambulances into service—"hospitals on wheels" staffed by two firefighters and a fourth-year medical student—initially intended to treat injured firefighters at fires and major accidents. In 1930, the service was extended to civilians injured at fires, explosions, and serious incidents. It was a hopeful turning point, but the timing was catastrophic.
The pattern that played out in Chicago between 1889 and 1928—municipal innovation driven by public need, followed by budget-driven compromise, fragmentation under competing priorities, and eventual collapse into a patchwork of inadequate alternatives—was not unique to one city. It was a preview of what would soon unfold nationally. What Chicago experienced across four decades, the rest of the country would experience in compressed form during the wars and Depression that followed. The difference was scale. Chicago's collapse left one city without adequate emergency medical transport. The national collapse would leave an entire generation of Americans relying on undertakers' hearses as ambulances.

American ambulance innovation did not stay within American borders. It taught the world.
The man who carried the lesson farthest was Dr. Benjamin Howard, a military surgeon trained in the Letterman tradition. Howard's initiation came at Antietam in 1862, when over ten thousand men lay on the field and, by the sudden disability of Dr. Letterman himself, supreme responsibility for their care fell to Howard by special order. From that baptism, Howard spent the next two decades refining ambulance design and field medical organization. His military ambulance won the highest international prize at the first Paris exposition, and was, by his own account, "largely used both in the American and Franco-German wars." 68,70 The Letterman lineage had produced not just an American system, but an exportable one—and the Franco-German War of 1870 was its first international proving ground.
But it was what Howard did next that revealed the full measure of American preeminence. In July 1881, Howard published a detailed account of the New York ambulance system in the British Medical Journal , presenting it as the standard London should aspire to.68 The system he described was not primitive. The Chief of Police served as de facto head of the ambulance system, in telephonic communication with a ring of hospitals whose buildings had been purpose-designed or retrofitted for ambulance operations. On the occurrence of any emergency, information was telegraphed to a central police headquarters, where an officer consulted a chart identifying the hospital district, and telephoned the call to the appropriate hospital. Horses stood harnessed around the clock. Ambulance surgeons filled out diagnostic blanks before attending to other duties, recording time of call, departure, arrival, return, and clinical details sufficient for a coroner's inquest. The ambulance, upon returning, entered through a porte-cochère into a reception ward supplied with operating tables, instruments, dressings, hot and cold water, beds, bathrooms, and small private rooms—all at a constantly agreeable temperature.68
Howard witnessed the system firsthand at New York Hospital . While he was speaking with the superintendent, their conversation was interrupted by a shrill whistle—a telephonic emergency call. Before Howard had finished putting on his hat, the superintendent had telephoned both driver and doctor, horses had been hitched to the ready ambulance, and the surgeon had departed at a gallop. Howard had nearly missed the performance the superintendent had asked him to witness. The ambulance, he noted, rivaled the fire department in speed of response. In every American city where the system operated—New York, Boston, Chicago, Philadelphia, Cincinnati, Washington—the ambulance had become as indispensable as the fire engine, and to abolish one would be as difficult as to abolish the other.68
That same month, a London surgeon named Samuel Stretton wrote to the British Medical Journal describing his attempt to transport his critically ill son—a medical student with diphtheritic throat—to the hospital. The only conveyance he could find, after considerable search, he described as "a cross between a hearse and dirty linen cart, painted black, and with funereal side glass; a black horse, with dismal harness, and a driver of the most woeful aspect, also in deep black."69 This was London in 1881—the capital of the British Empire—while American cities had integrated physician-staffed ambulance systems with two-minute response times.
Howard did not merely describe what America had built. He went to London to build it for them. In January 1882, he presented a comprehensive proposal to the Medical Society of London , published in The Lancet , in which he surveyed American systems in six cities, demonstrated a purpose-built ambulance he had designed and had constructed in London for the London Hospital , and outlined a district-based coverage system linking police stations by telegraph and telephone to a central hospital. The ambulance he presented—the only accident ambulance carriage belonging to a general hospital in civilian Europe, by his account—incorporated the same counterpoise spring system he had designed for his military ambulance, the one used in the Franco-German War. He had carried the Letterman lineage from Antietam to Paris to London in a single career.70
By 1884, the American model was spreading. An Edinburgh physician, Dr. Peter Alexander Young, wrote in the Edinburgh Medical Journal that "as in many other practical points, our American cousins have been ahead of us in the matter of ambulance organization." Howard's pattern ambulance wagons had been supplied to London police stations at Stoke-Newington, Fulham, and Lambeth; to Liverpool's Northern Hospital , where a resident ambulance surgeon stood on duty around the clock; and to ambulance associations across Scotland. Glasgow and Edinburgh had organized trained ambulance corps modeled on the American system, with telephonic dispatch and Howard-designed vehicles.71
But one line in Young's account is telling: "Unfortunately, the London hospitals have not joined in any way in the movement." The ambulances were going to police stations, not hospitals. The knowledge had been transferred. The equipment had been deployed. The institutions refused to own it. Twenty years later, nothing had changed. In March 1904, a London physician named W. Atterbury wrote to the British Medical Journal describing his difficulty procuring an ambulance for an acute appendicitis case, noting that London's ambulance service remained "in a very unsatisfactory state." He had to send to Edmonton and endured "considerable delay." His plea was identical to Howard's a generation earlier: there should be an ambulance in every district of London, available for non-infectious cases on the application of a medical practitioner.72
The lesson is not that the British were slow to learn. The lesson is that even the direct transfer of the world's most advanced ambulance system—hand-delivered by a practitioner trained in its founding tradition, with purpose-built equipment, published protocols, and documented results—could not sustain itself without the institutional commitment to maintain it. If London could not hold what America gave it, the fragility of America's own systems becomes less surprising. The pattern that would destroy American EMS in the decades ahead was already visible: build something sophisticated, watch it spread, then watch it starve when the institutions meant to sustain it lose interest.
The export of American ambulance capability continued to accelerate. By the First World War , it was massive. The American Red Cross , the Norton-Harjes Ambulance Corps , and the American Field Service deployed hundreds of American ambulances and medical personnel across France and Italy. The service was not without cost: 296 Red Cross nurses and 127 ambulance drivers died in the war.13
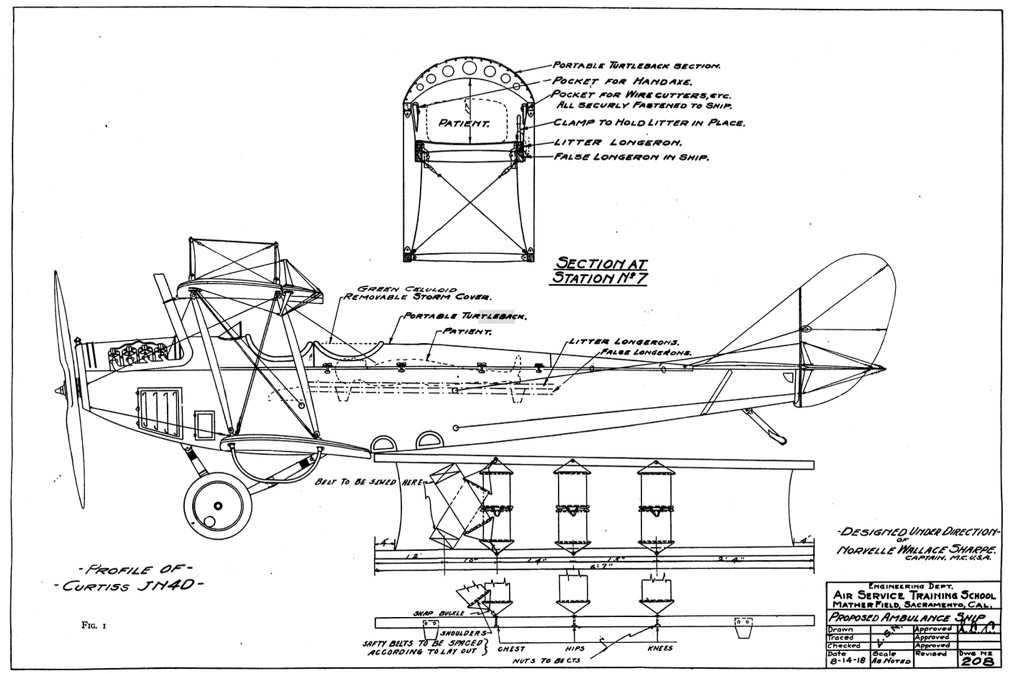
Innovation accelerated in parallel. In 1918, proposals were advanced for ambulance aircraft using modified JN-4D biplanes—the air medical concept articulated decades before anyone had the technology to implement it.14 In 1928, the Washington, D.C. Fire Department integrated ambulance services into its fire-based operations, establishing an early model of fire-based EMS.15 That same year, the Roanoke Life Saving Crew in Virginia organized as the first sustained volunteer rescue squad in the nation.16 By 1937, Hess & Eisenhardt in Cincinnati had built the first air-conditioned ambulance.17
The Roanoke crew was not alone. By the 1930s, organized volunteer first aid and rescue squads had proliferated across states like New Jersey, where 347 squads eventually provided free statewide ambulance and first aid coverage.33 These were trained, equipped, community-funded organizations with structured leadership, cooperative coverage agreements, and municipal financial support. The pre-war landscape of American emergency medical services was not a single model, rather it encompassed physician-staffed municipal ambulances in major cities, hospital-based services, fire department operations, and organized volunteer squads. What unified them was institutional seriousness: training standards, dedicated equipment, and deliberate community investment.
And then came the high-water mark.
In November 1938, a joint committee of the Chicago Medical Society, the Chicago Hospital Council, the American College of Surgeons, and the Chicago Council of Social Agencies published a proposal for a comprehensive public ambulance system. The committee, chaired by Dr. Malcolm T. MacEachern, Associate Director of the American College of Surgeons, declared that “Chicago is the only large city in the United States” that lacked “one medically adequate public ambulance available for general emergency use.”18
The language used here is precise and worth pausing over. The committee did not call for more ambulances.
It did not call for faster transport.
It did not call for lower standards.
It called for medically adequate ambulances. Ambulances that are funded, staffed and equipped to deliver physician-directed clinical care in the field.
In 1938, the institutional standard being demanded for Chicago was not a ride to the hospital. It was out-of-hospital medicine.
Now, the committee had reason for alarm. Chicago’s first six motorized fire department ambulances had been built in 1928, staffed by two uniformed firemen and a fourth-year medical student, and described at the time as “hospitals on wheels.” But by 1937, five of the six had been pulled from service due to Depression-era budget cuts. Two were transferred to the Board of Health’s Contagious Disease Hospital. Only ‘Ambulance 1’ at ‘Engine 1’ remained in frontline service. Chicago, a city that once was in a race to implement the nation’s best ambulance service, now had just one ambulance for a city of over three million people, and that one was restricted to care for injured firefighters.34 Before the fire department had entered the ambulance business in 1928, Chicagoans who needed emergency hospital transport had three options: drive the patient themselves, rely on the police patrol wagon—the infamous “black maria”—or call the local undertaker.34 The MacEachern committee was not proposing something unprecedented. They were trying to restore what the Depression had already begun to destroy.
The standard the committee articulated was medical adequacy, not mere transport. The proposal called for a minimum of twenty ambulances housed in or adjacent to hospital-approved facilities, deployed across the city based on “density of population, industrial centers, accident and emergency frequency, and the location of ambulance hospitals.” It proposed emergency care for indigent patients at all private hospitals, with reimbursement “in part, at least, for such service by the city, the relief administration, and other social agencies.” It included a detailed budget: $173,300 for the first year, with $130,700 for subsequent annual operations.18
Read those specifications carefully. Zoned deployment based on population density and emergency frequency. Hospital-integrated ambulance stations. A reimbursement structure for indigent care. Operational budgets at the municipal level. This is the vocabulary of 1970s EMS system design, but this was written thirty years before the 1966 White Paper that is conventionally credited with inventing it.
The 1938 proposal was a plan, backed by the American College of Surgeons , with a budget and a timeline.
Tragically, the realities of war killed it before implementation.
But the full measure of what would be lost is best understood through the institution that held on longest. The ambulance staffing model that Bellevue established in 1869—a physician plus a driver—would endure in New York City for nearly a century. When World War II stripped physicians from the ambulances in February 1942, public outcry forced their reinstatement by November 1948. The model survived until 1962, when the Department of Hospitals finally replaced physicians with minimally trained ambulance attendants. The transition was not because of a wartime emergency, but because of liability insurance costs and rising call volumes approaching 400,000 per year.8,36 Read that timeline again. From 1869 to 1962—through two world wars, the Great Depression, and the postwar boom—New York City maintained an institutional commitment to placing physicians on ambulances. When it finally ended, the cause was not a crisis of capability but a crisis of cost. The change came with a fundamental redesign of the ambulance’s purpose: from a system designed to bring medical care to the patient, to one built to bring the patient to medical care. The mission shifted from treatment and transport if necessary, to a lower cost transport-centric model. The transport-centric model, once adopted, proved to be less expensive and easier to staff than the clinical model it replaced.

A final observation before the darkness falls.
Today, global EMS is broadly divided between two competing models: the Anglo-American system, built around the paramedic, and the Franco-German system, which places physicians on ambulances. The two are typically discussed as parallel traditions with separate origins. But the American ambulance systems of the 1860s and 1870s were physician-staffed—and it was precisely this model that the United States exported to Europe through military aid and wartime ambulance deployments over the next half-century. When German and French medical leaders formalized physician-staffed ambulance systems in the late 1950s and 1960s—what scholars describe as “reviving” the concept of bringing the doctor to the patient—they were building on a foundation that American cities had laid nearly a century earlier.
What Europe preserved, America lost during the Dark Age.
When the American ambulance rebuilding era came, it did not restore the old model, but it again created something new: the paramedic, a role without historical precedent, designed to bring advanced clinical capability to the field without requiring a physician on every ambulance. That innovation was genuine and consequential. But the institutional and financial architecture that had supported the older system was never rebuilt to support the new one. The paramedic was a breakthrough. The infrastructure around the paramedic was a compromise.
The paramedic was a breakthrough. The infrastructure around the paramedic was a compromise.
Chapter 3 — The EMS Dark Age (1939–1958)
World War II did not merely pause the development of civilian emergency medical services. It caused an active regression—a collapse so thorough that it took decades to recognize what had been lost, and from which the profession has never fully recovered.
The wartime mobilization of medical personnel was total. Physicians, surgeons, and trained ambulance attendants were redeployed to military service or reassigned to hospital-based care that served the war effort. Civilian ambulances—most, though not all of them—reverted to transport-only vehicles with no medical care provided en route. The regression was abrupt; in city after city, ambulances that had carried physicians for generations were suddenly crewed by whoever could be found to drive the ambulance.
The Great Depression of the preceding decade had already weakened municipal ambulance budgets, thinning the infrastructure that might have withstood the shock. Chicago’s experience was illustrative. The city’s six fire department ambulances—staffed by firefighters and medical students, equipped as mobile treatment units—had been reduced to a single vehicle by 1937, years before the first soldier shipped overseas.34 When the war arrived, the fire department had only begun rebuilding: two Packard ambulances were placed back into frontline service in April 1942, operated by Civil Defense and staffed by civilians.34 By June 1942, there were still only six fire department ambulances for the entire city, with the Chicago Police Department handling the balance of all medical calls. After the war, in November 1945, ambulances were once again staffed by firefighters and service was extended to civilians—but private ambulance companies immediately complained that the fire department was cutting into their business, and an order was issued requiring a division marshal’s authority to dispatch a CFD ambulance.34 The infrastructure had been so thoroughly hollowed out that even restoring basic service triggered jurisdictional resistance.
When the war stripped away the remaining clinical personnel, there was no reserve capacity to absorb the loss.
The parallel to the fall of Rome is more than rhetorical. When the Roman legions withdrew from the provinces, the roads and aqueducts they had built did not immediately crumble, but the knowledge and institutional capacity required to maintain them evaporated. Within a generation, communities that had enjoyed running water, engineered roads, and organized public services were left with crumbling ruins they could see but could not replicate. The same dynamic unfolded in the American EMS system. The vehicles still existed. Some of the buildings still stood. But the clinical mission that had defined them—the expectation that an ambulance was a medical vehicle crewed by medical professionals, as a funded core city service—simply vanished.
The collapse of clinical capability might have mattered less in a static world. But the mid-twentieth century was anything but static. The industrial revolution, the expansion of the American highway system, and the rapid growth of cities were accelerating the frequency and severity of medical emergencies at precisely the moment the system designed to respond to them was disintegrating.

What filled the vacuum was the funeral industry.
By the 1950s, funeral homes were the primary ambulance providers across much of rural and suburban America. The logic was grimly practical: funeral homes owned the only vehicles with wheelbases long enough to accommodate a stretcher. They operated around the clock. And they had a workforce—funeral directors and mortuary attendants—who were, at minimum, accustomed to handling human bodies.19
What they did not have was specialized medical training. It was a far cry from the ambulance surgeon physicians that had staffed ambulances decades prior. As a postwar analysis summarized it: “Postwar ambulances were underequipped hearses and similar vehicles staffed by untrained personnel. Half of the ambulances were operated by mortuary attendants, most of whom had never taken even a first aid course.”20
That assessment is retrospective. But the conditions it describes were documented in real time. In 1951, writing in the National Municipal Review, Schubert and Marling observed that “in most of the country people are living under frontier conditions so far as the availability of ambulance, first aid and rescue service is concerned.”33 Frontier conditions. Not a retrospective judgment rendered decades later, but a contemporaneous assessment published in a peer-reviewed municipal governance journal at the height of the Dark Age itself.
The vehicles themselves told the story. “Combination cars” became the standard—vehicles engineered to switch between hearse and ambulance function with minor modifications.21 The same car that carried a casket to a cemetery on Saturday morning might carry a heart attack patient to a hospital on Saturday night. By the 1960s, over half of America’s ambulances were not purpose-built medical vehicles.19 In Chicago, the pattern was visible at ground level: local undertakers, already on call around the clock, used their combination hearses as ambulances when not carrying the dead. The equipment in these vehicles was typically sparse—a stretcher, a blanket, and a first aid kit or tackle box filled with gauze and bandages.34 Compare that to what Chicago’s police ambulances had carried in 1889: tourniquets, splints, disinfectant, an emetic protocol, environmental medicine supplies. The degradation was not abstract. It was measurable in the contents of the vehicle.
The incentive structure was perverse. Funeral homes that arrived first at accident scenes often secured the funeral business if the patient died. Stories of hearses racing each other to crash sites became commonplace in rural communities—not because the drivers were eager to provide care, but because the first to arrive captured the downstream revenue.22 The emergency medical call was, functionally, a sales lead. Schubert and Marling documented the practice firsthand, reporting that in Syracuse, morticians maintained “dual-purpose vehicles, part hearse and part ambulance,” and that in Memphis, “ambulance hearses driven by morticians raced each other to accidents for the purpose of soliciting funeral business.”33
From physician-staffed, purpose-built vehicles dispatched by telegraph, integrated into hospital systems, and funded by municipal budgets—to combination cars driven by mortuary attendants scanning police radios for accident reports. That trajectory, compressed into roughly fifteen years, is the Dark Age in miniature.
From physician-staffed, purpose-built vehicles dispatched by telegraph— to combination cars driven by mortuary attendants scanning police radios for accident reports.
And it was not an interim measure. It became the normalized model for more than twenty years. An entire generation of Americans grew up believing that this was what ambulance service was supposed to look like.
Perhaps the most powerful evidence of the Dark Age is the evidence that does not exist.
My EMS Development Timeline—a freely accessible research project I published in 2023 after working on it for more than a decade, cataloguing significant milestones in the history of emergency medical services with primary source documentation and links—contains a conspicuous void between approximately 1939 and 1956. It was not until recently that this gap became evident and pronounced. The entries before that period are dense and varied: new ambulance services, technological innovations, clinical standards, international programs, institutional investments. The entries after 1956 resume with increasing intensity. But between those dates, the record goes nearly silent.
This void is itself diagnostic. Innovation requires investment, and investment had ceased. The absence of milestones is not a gap in the research. It is the research finding.
The silence was not quite total. One institution maintained a thread of continuity through the darkness: the American College of Surgeons. The ACS Committee on Trauma—which had begun as the Subcommittee on Ambulance Equipment in the Emergency Treatment of Fractures in 1931—continued publishing equipment standards, splinting guidelines, and training recommendations throughout the Dark Age period.35 In 1936, the subcommittee recommended basic ambulance equipment lists and responder training. By 1949, it had been renamed the Subcommittee on the Transportation of the Injured and was calling for ambulance attendants to transition from transporters to caregivers. In 1961, it published a minimal equipment list for ambulances.35 But this continuity makes the Dark Age more damning, not less. The knowledge was being maintained. The standards were being published, but across most of the country, they were being ignored. The ACS was a monastery copying manuscripts that no one outside the walls could read.
The silence becomes even more striking when contrasted with what was happening internationally. When Dr. Peter Safar visited the Soviet Union in 1963, he discovered that the Soviets had maintained and advanced purpose-built ambulance systems throughout the period when Americans were still dispatching repurposed hearses.23 The Cold War rival had preserved what America had abandoned.

1950s Soviet era purpose built ambulances.
Here lies the central paradox of the Dark Age: the same wars that produced extraordinary advances in trauma care, battlefield evacuation, and resuscitation simultaneously destroyed the civilian systems that should have been the beneficiaries of those advances. Military medicine leapt forward. Civilian emergency medicine collapsed, and when the wars ended, the military lessons sat unused for years—sometimes decades—because the civilian infrastructure that should have absorbed them no longer existed.
Who preserved the knowledge of emergency medicine through the Dark Age? If this parallel holds, were there monasteries—institutions or individuals who kept the flame alive when everything around them had gone dark?
There were a few.
In 1956 and 1957, Peter Safar and James Elam validated the technique of mouth-to-mouth resuscitation—foundational science that, remarkably, also was lost and had to be rediscovered.24 The implications of that word are worth pausing over. A technique essential to saving human lives had fallen out of clinical practice and scientific validation to such a degree that it required formal re-establishment.
Then, in 1958, Dr. J.D. “Deke” Farrington and Dr. Sam Banks posed the question that defines this entire book: Why aren’t the lessons of battlefield trauma care being applied to civilian emergencies?25 Farrington did not wait for someone else to answer. In the aftermath of World War II and the Korean Conflict, he and Banks launched the first civilian trauma training course for…the Chicago Fire Department! The physicians, yet again, chose to adapt military field medicine to urban emergency response. The course became the foundation for the EMT-Ambulance certification and laid the groundwork for structured, medically supervised EMS training nationwide.25
Dr. J.D. Farrington teaching EMT class, 1950s.
Farrington’s question was not a visionary’s dream of a future system. It was a witness’s recognition that a present system had failed—that knowledge which existed and had been proven was not being used. He was standing inside the Dark Age and naming it.
In 1959, the American Medical Association published a landmark report, prepared at the request of the White House, warning of “inadequately trained personnel with poor equipment.”26 The report documented what Farrington already knew: the civilian emergency medical system was broken. But the scale of the problem was only beginning to come into focus.

Chapter 4 — The Incomplete Renaissance (1958–1970s)
The reformers who rebuilt American EMS in the 1960s and 1970s are rightly honored as visionaries. They saw a crisis that most of the country had learned to ignore, and they built systems where none appeared to exist. But the conventional narrative gives them credit for the wrong thing. They did not invent emergency medical services in America. They recovered EMS in America, but imperfectly, and from a lower baseline than what was envisioned and established nearly a century prior.
Farrington’s training course and the AMA’s 1959 report had sounded the alarm. But diagnosing the crisis and rebuilding the system were two different things. The rebuilding, when it came, would be shaped less by what the reformers knew than by what they did not know—namely, how much had existed before.
The White Paper: Rediscovery Disguised as Discovery
In 1966, the National Academy of Sciences published Accidental Death and Disability: The Neglected Disease of Modern Society—the document universally recognized as the founding charter of modern EMS.27 Its findings were devastating. Its call to action was urgent, and it changed the trajectory of emergency medical services in the United States.
But read through the lens of the Dark Ages, the White Paper takes on a different character. It reads not as a bold discovery of something new, but as an anguished recognition of something lost. The conditions it documented—untrained ambulance crews, inadequate equipment, no medical oversight, no communication systems, no standards—would have been unrecognizable to practitioners of the 1880s and 1890s who had built physician-staffed, telegraph-dispatched, hospital-integrated ambulance services decades earlier.
The White Paper reads not as a bold discovery of something new, but as an anguished recognition of something lost.
The report’s own language is revealing. It describes ambulance service as a “neglected” problem, as if it were a public works project that had been allowed to deteriorate through inattention. But it was not merely neglected. It had been actively destroyed—first by the Depression, then by the comprehensive wartime reallocation of medical personnel—and then replaced by a degraded substitute that persisted so long it became the norm. The word “neglected” implies something forgotten in a corner. What happened to civilian EMS was closer to demolition.
The same year, the Highway Safety Act placed EMS under the Department of Transportation.28 The institutional logic made sense at the time: highway fatalities were the crisis that had generated political will. But, the framing shaped EMS’s identity for decades. Emergency medical services was becoming a transportation issue rather than a healthcare issue, a framing that still shapes reimbursement structures, regulatory frameworks, and professional recognition. The bias was not merely conceptual, but it was largely geographic. The Highway Safety Act’s focus on rural highway fatalities meant that urban ambulance systems, which had their own distinct crises, were less emphasized in the initial federal response. Congress attempted to correct the imbalance in 1973 with the Emergency Medical Services Systems Act, which sought to build comprehensive, regionalized EMS networks. But rather than replacing the earlier framework, the new law created a second, competing federal mandate: one housed in the Department of Health, Education, and Welfare while the original remained under the Department of Transportation. The result was not a unified national EMS architecture but two parallel federal authorities with overlapping jurisdiction and divergent priorities, a fragmentation that compounded the structural incoherence the legislation was meant to resolve.37
The competing mandates proved short-lived. In 1981, the Omnibus Budget Reconciliation Act consolidated EMS funding into state-administered block grants, eliminated the designated lead federal agency for EMS within the Department of Health and Human Services, and repealed most of the Emergency Medical Services Systems Act.38 The plan for three hundred, nationally designated, funded and coordinated regional EMS systems — the central promise of the 1973 Act — was abandoned. State EMS offices, many of which had existed for less than a decade, lost their federal funding overnight and were left to compete with other health and social programs for a share of diminished block grant allocations. Without unified federal standards or dedicated funding, states diverged rapidly. Each developed its own certification levels, training requirements, and examination standards. By the 1990s, the United States had more than forty documented variations of EMT certification, each with distinct knowledge and skill requirements. This was a fragmentation so severe that EMS professionals often could not transfer credentials across a state line without re-taking classes or licensure examinations. The national system the founders had envisioned did not fail because it was poorly conceived. It failed because the federal government built it, then walked away from it within a decade. The fragmentation that defines American EMS in 2026 (the inconsistent credentialing, the workforce immobility, the fifty separate regulatory architectures) traces directly to that abandonment.
The national system the founders had envisioned did not fail because it was poorly conceived. It failed because the federal government built it, then walked away from it within a decade.
How deep was the void the reformers faced? In 1969, three years after the White Paper, the U.S. Department of Health, Education, and Welfare published a compendium of every state statute governing ambulance services in the United States. The summary was damning in its sparseness. Only four states required registration of ambulance vehicles or services. Only eleven had any qualification standard for ambulance personnel. Only five required two crew members on an emergency run. Only two required any record-keeping for patients. The majority of states that addressed ambulances at all did so only in traffic code, classifying them alongside fire trucks and police cars for the purpose of siren exemptions and speed limit waivers. Several states' only relevant statute was a provision exempting funeral cars and ambulances from regulation as common carriers. The document did not describe a profession in crisis. It described a profession that did not yet legally exist.51
Consider the distance the profession had fallen. In 1895, police officers assigned to Chicago’s ambulances were performing tourniquet application for traumatic amputations, hemorrhage control by protocol, and structured patient assessment. The medical skills they described in detail to a Chicago Tribune reporter who spent a day observing their work.34 In 1938, the American College of Surgeons demanded “medically adequate” ambulances housed in hospital-approved facilities with zoned deployment, indigent care reimbursement, and detailed operational budgets.18 Yet, by 1966, the Department of Transportation was conducting a national survey to determine how many funeral home hearses, pulling double duty as ambulances, had drivers with basic first aid training.29
From tourniquet application, medical protocols, and hemorrhage control to a census of who among the hearse drivers had taken a community level Red Cross course. The bar had not just been lowered. It had been buried.
The bar had not just been lowered. It had been buried.
The timing makes the regression even starker. In 1962, four years before the White Paper sounded the national alarm, New York City’s Department of Hospitals quietly ended the last routine physician staffing on municipal ambulances, replacing the remaining ambulance surgeons with minimally trained attendants. The stated reason was not a lack of physicians but the rising cost of liability insurance and the strain of call volumes approaching 400,000 per year.36 The city that had invented the physician-staffed ambulance in 1869—that helped export the model globally, had fought to restore physician staffing after World War II and succeeded in 1948—surrendered the model permanently not in wartime but in peacetime. The model was ended not for lack of knowledge, evidence, or patient outcomes, but for the lack of will to fund what it had always known was necessary. The reformers of the late 1960s were not merely rebuilding from a collapsed past. They were rebuilding while the last remnants of the old standard were still being dismantled around them.
The Foundational Compromise
In the urgent rush to rebuild EMS in the late 1960s and 1970s, the nation’s leaders made a series of pragmatic compromises that were intended to be temporary but became permanent.
The rapid expansion of EMT training—standardized at roughly 140 hours—was designed as a minimum viable standard, a floor from which the profession would rise. It was not intended to be a ceiling. But it calcified into one. The staffing model shifted permanently from physicians to non-physician providers—a change born of wartime necessity but validated by what came next. The paramedic, as Freedom House would prove, was not envisioned or created as a lesser substitute for the physician on the ambulance. It was a new clinical role, rigorously trained, operating under physician oversight, capable of delivering advanced care that the old model had never attempted in the field. The problem was not the paramedic. The problem was that the nation built this new profession on top of the Dark Age’s broken financial foundation and never replaced it. When Medicare’s reimbursement structures took shape after 1965, they were built around the concept that ambulances provided transportation to medical care, rather than providing clinical care. This unfortunately permanently encoded the Dark Age’s transport-only model into the federal payment architecture that persists to this day.30
However, there were some brilliant exceptions, and one of these exceptions became the contemporary blueprint for the modern paramedic.

In 1967, the Freedom House Ambulance Service began operations in Pittsburgh’s Hill District. This was a predominantly Black neighborhood where residents in medical crisis were more likely to receive a police wagon than an ambulance, and where response times reflected the city’s racial geography. Dr. Peter Safar, the University of Pittsburgh anesthesiologist already known as the “Father of CPR,” designed an intense 32-week training program. His new paramedics included people who had experienced chronic unemployment and veterans of the Vietnam War. Leveraging his authority as a world-renown anesthesiologist and critical care pioneer, combined with the medical direction of Dr. Nancy Caroline, Freedom House paramedics were trained as physician extenders. They would perform advanced procedures in the field that no other non-physician healthcare providers in the country were permitted to do: intubation, cardiac care, intravenous drug administration.31
The results were dramatic and immediate. In the first year, this new ambulance service responded to approximately 5,800 calls and saved 200 lives.31 The curriculum Caroline developed for Freedom House was adopted by the federal government in 1975 as the first national paramedic curriculum. Separately, her textbook, Emergency Care in the Streets, became the standard paramedic textbook worldwide. The ambulance design that Safar refined through Freedom House operations, informed by what he had seen in the U.S.S.R., became the NHTSA standard. Miami, Los Angeles, and Jacksonville, all experimenting with their own paramedic programs, would join forces to advance the Freedom House model. The paramedic, as a defined professional role with standardized training and clinical protocols, exists in its modern form because of what was demonstrated in the Hill District.31 Freedom House effectively solved the clinical problem. What it could not solve, and what no single program could solve, was the financial architecture that would have made its model sustainable.
Freedom House proved that the foundational compromise was not inevitable. They proved that advanced prehospital care could be delivered by rigorously trained non-physician providers working in collaboration with physician oversight, even in communities that the existing system had abandoned. But the program also demonstrated how fragile progress remained. Despite its national influence, Freedom House was defunded in 1975 when Pittsburgh’s city government launched its own ambulance service. Most of the Black paramedics who had pioneered the model were excluded from comparable positions in the replacement system.31 The nation adopted Freedom House’s curriculum, its ambulance design standards, and its clinical model—and then let the program itself die. Freedom House thus embodies the central paradox of this entire book: clinical innovation without financial architecture produces brilliance that cannot sustain itself. The program’s clinical legacy is permanent. Its institutional legacy is a cautionary tale. Both lessons matter equally. The pattern should by now be familiar.
Chicago’s experience during this period illustrated both the promise and the limitations of the rebuilding effort. In 1970, the federal government funded eleven “Model Cities” ambulances for Chicago—inexpensive Ford club wagons that performed poorly. The firefighters assigned to them earned $7,500 to $8,500 a year. The program lasted only one year, but it produced a new CFD record of 81,956 runs—a surge in demand that exposed how thoroughly the system had been starved of capacity.34 When the federal government finally established standards for modular ambulances in 1973, Fire Commissioner Robert Quinn resisted the transition from his department’s beloved Cadillac ambulances, reportedly on the theory that “a Chicagoan would rather die in style than be saved in the back of a panel truck.”34 Quinn’s attachment to the Cadillacs—beautiful vehicles that were clinically inferior to the modular designs with their greater interior space and capacity for life-saving equipment—embodied a subtler dimension of the Dark Age’s legacy:
institutional nostalgia for a compromised framework that had persisted so long it felt like tradition.
The compromises themselves were rational given the depth of the crisis. No reasonable person standing in 1966 would have insisted on perfection when people were dying for lack of any care at all. The failure was not in making the compromises. The failure was in never going back to finish the work. The failure was treating emergency measures as permanent architecture, in confusing the floor with the ceiling, in allowing the expedient to become the expected.
The greatest failure was not in making the compromises. The failure was in never going back to finish the work.
Chapter 5 — Are We Still in the Dark Ages?
If my argument is correct—
that the chronic structural problems of American EMS are not growing pains of a young profession but the inherited consequences of a mid-century collapse and an incomplete recovery
—then the question is not whether the Dark Ages ended, but whether we have yet achieved a true renaissance.
Return to South Dakota.
The state has gone from 131 ambulance services to 121 in a single decade.1 Its average EMT is 52 years old.2 It has 28 active EMTs between the ages of 70 and 75, and two in their eighties. The state is purchasing power cots so that aging providers can physically lift patients into ambulances.2 Medicare reimburses approximately $650 per ambulance run in rural areas; Medicaid pays roughly $400. The cost to operate the ambulance response exceeds both figures. A 2023 consultant’s report recommended state funding for ambulance services, but three years later, no such funding has materialized.1
South Dakota's financial crisis is not an anomaly. It is the national condition. EMS has never been financially self-sustaining. Not in 2026, not in the 1970s, and not even when funeral homes ran it. In 1969, 221 funeral homes provided ambulance service in Oklahoma; by 1973, the number had dropped to 124, a forty-four percent decline, because the economics of providing the service could not support even the funeral industry's low-overhead model. When Congress passed the Emergency Medical Services Systems Act of 1973, it identified fifteen essential components of an EMS system (regulation, medical direction, communications, transportation, patient care) but deliberately omitted a sixteenth: sustainable financing. The assumption was that state and local governments would eventually find a solution. They did not. A half-century later, independent financial analyses in multiple states have reached the same conclusion: absent a subsidy, no transporting EMS agency in the United States can break even.
Maine's 2022 Blue Ribbon Commission55 found that every transporting EMS service in the state was operating at a loss, from a required subsidy of $322 per transport for high-efficiency urban services to $2,030 per transport for low-volume rural ones. The most significant subsidy masking this insolvency for decades has been volunteer and underpaid labor. The current crisis is not that EMS is becoming insolvent. It is that the decline in volunteerism is revealing what was always true: communities built on volunteer EMS never knew what it actually cost because they were never paying for it.39
In 1975, the U.S. Department of Agriculture published a study of rural ambulance service in the Great Plains, documenting that funeral home operators were abandoning ambulance service across Oklahoma due to rising costs, that a fully staffed EMS system would require annual subsidies of $15,000 or more per county, and that only systems dependent on modestly paid volunteers could operate without public subsidy. The report's conclusion was precise: communities that wanted professional EMS would have to pay for it. In 1986, the GAO said the same thing. Maine documented it again in 2022. In April 2024, the New York State Comptroller issued a report announcing that ambulance companies and EMS divisions across the state were struggling with low pay, reliance on volunteers, and increasing patient volumes, and that the financial burden was increasingly falling to county governments funded by property taxpayers. The report was presented as a discovery. It was not. The economics of EMS have not changed in fifty years. What has changed is the willingness of volunteers to mask them.50

The evidence is no longer in dispute. Independent analyses spanning fifty years, conducted in different states by different investigators using different methodologies, arrive at the same conclusion: the financial model underlying American EMS does not work, has never worked, and cannot be made to work through incremental adjustment. The question that demands an answer is no longer whether the system is failing. It is why the same failure keeps being rediscovered, decade after decade, as though it were new. That question requires examining not the symptoms but the architecture—the foundational decisions about how emergency medical services would be funded, classified, and positioned within the American system of public services. Those decisions, and their consequences, are the subject of the next chapter.
Chapter 6 — The Architecture No One Chose
Chapter 5 documented the evidence. The funding model is broken. Every independent analysis confirms it. But broken is not an explanation. Models do not break without a reason, and the reason matters, because it determines whether the repair is possible or whether the model itself must be replaced. The financial architecture of American EMS—the reliance on individual patient billing as the primary revenue mechanism for a public safety function—was not chosen deliberately by anyone who understood its consequences. It was not the product of policy analysis, stakeholder consensus, or comparative study. It was the consequence, the residual outcome of a jurisdictional contest between two federal agencies in the 1960s, a self-sufficiency requirement embedded in the 1973 EMS Systems Act, and the collapse of federal healthcare funding for EMS in 1981. The profession inherited a funding model the way a family inherits a house built on a floodplain: not by choice, but by circumstance, and the flooding has been predictable ever since.
The financial failure is real, but it is a symptom of something more fundamental: a conceptual misclassification that no amount of reimbursement reform can fully correct as long as the underlying assumption remains intact.
Consider how America funds its other essential public services. Police departments do not bill the victims of crime for the responding officers. Fire departments do not invoice homeowners for the cost of suppression. Public schools do not charge tuition. School buses do not collect fares from students. Roads, water systems, sewer infrastructure, and public libraries are funded through the tax base because American society long ago accepted a foundational principle: services that exist for everyone must be paid for by everyone. The cost of readiness — maintaining the infrastructure, staffing it, equipping it, and ensuring it is available twenty-four hours a day whether anyone uses it on a given Tuesday or not — is distributed across the tax base because the alternative is both inefficient and unjust.
EMS operates under a fundamentally different premise. The primary revenue mechanism for most ambulance services in America is not public funding. It is a bill generated when someone calls for help. The cost of readiness — the ambulances, the personnel, the training, the ceaseless availability — is not distributed equally across the community. It is loaded onto the individual patients who happen to need the system on any given day. Every resident of a municipality benefits from knowing that an ambulance will respond if they collapse in their kitchen tonight. But only the person who actually collapses receives the bill. In effect, the American EMS financing model takes a public safety function and funds it like a private transaction.
The distributional consequences are predictable and severe. The population that generates the highest volume of EMS calls is disproportionately elderly, low-income, chronically ill, and un- or underinsured. This is precisely the population least able to absorb the cost. Medicare and Medicaid reimburse below the cost of service. Uninsured patients generate bills that are rarely collected. But the distortion does not end with the patients who cannot pay. It is compounded by what happens to those who can.
The scale of this shortfall is not speculative. A 2012 analysis by the National EMS Advisory Council, revised and reaffirmed through 2019, estimated that ground ambulance services in the United States absorb approximately $2.9 billion in uncompensated care annually — roughly half the total amount Medicare paid to all ground ambulance services nationally. Ambulance providers receive below-cost reimbursement on 72 percent of all transports: the combined burden of charity care delivered to the uninsured and under-compensated care from Medicare and Medicaid rates that do not cover the cost of service.58
Middle-class and insured patients routinely receive ambulance bills grossly disproportionate to the services they individually received, because the billing structure must recover not only the cost of their own care but the uncollected costs of every patient who could not or did not pay before them. The result is that the segment of the population most capable of generating political pressure — working families who open a four-figure bill for a fifteen-minute transport — is the segment most likely to conclude that the system is predatory.
And maybe they are not wrong?
They are simply encountering, at the individual level, the consequences of a public financing failure that should never have reached their mailbox. The cultural backlash was severe enough to produce federal legislation. The No Surprises Act, signed into law in 2021, prohibited most surprise medical billing from out-of-network providers, but notably excluded ground ambulance services from its protections. Congress acknowledged the problem, wrote a law to address it, and carved EMS out. A separate federal advisory committee was established to study the ground ambulance billing question, effectively deferring the issue while every other category of surprise medical billing was resolved. The message was unmistakable: even in legislation specifically designed to protect patients from disproportionate medical bills, EMS occupied a category so structurally dysfunctional that Congress could not apply the same remedy it applied to everyone else. The public is not angry at EMS. The public is angry at being asked to personally subsidize what every other essential public service funds collectively. The funding model that asks the most vulnerable people in a community to serve as its primary financiers simultaneously alienates the people with the political influence to change it. It is a cost-shifting arrangement in which the sick subsidize the healthy, the insured subsidize the uninsured, and the gap between what the system costs and what patients can pay is filled — when it is filled at all — by volunteer labor, municipal appropriations, bake sales, and the quiet personal bankruptcy of the agencies themselves.
This is what happens when a medical profession is rebuilt on a transport model rather than a care model. The decision to define the ambulance response as a billable transport event rather than a public safety deployment was not inevitable. It was a policy choice, made incrementally across decades, and it carries a structural consequence that no adjustment to the Medicare fee schedule can resolve. As long as EMS is financed as a transaction rather than funded as infrastructure, the economics will remain broken: not because the reimbursement rate is wrong, but because the entire premise is.
The misclassification is encoded into federal regulatory structure. Medicare classifies ambulance services as suppliers of transportation, not providers of healthcare. This is the designation that determines reimbursement methodology, conditions of participation, and institutional standing within the federal healthcare system. The same NEMSAC advisory that documented the $2.9 billion uncompensated care burden conducted a formal analysis of EMS functions by discipline and concluded that healthcare functions exceeded any other discipline by a nearly three-to-one margin.58 The federal government's own advisory council determined that EMS is predominantly a healthcare function, yet the federal government's own payment system continues to classify it as transportation.
And in January 2026, the South Dakota legislature's proposed remedy included a bill to allow individuals trained only in CPR to operate ambulances. 1 Compare that directly to the 1950s, when untrained personnel replaced the physicians who had been called to war. The parallel is not metaphorical. It is operational.
South Dakota is one example, but the structural deficiencies it illustrates are national. EMS remains the only major component of the American emergency response system without a dedicated federal funding stream. Fire departments have one. Law enforcement has one. Emergency Management and disaster preparedness are funded. Schools, garbage collection, social services, parks and recreation . . . are all tax-base funded in nearly every community in the United States. Yet, EMS is systemically neglected and remains non-essential. Medicare still primarily reimburses EMS for transport, not for clinical intervention. This is the Dark Age’s transport-only model encoded into payment policy and never fundamentally reformed.30 The scope-of-practice debates that consume the profession—what EMS clinicians should be permitted to do—are not reflections of the paramedic’s inadequacy but of a regulatory and financial framework that was never designed to support what the paramedic can actually deliver.32 The floor that was supposed to be temporary became the ceiling, and any attempt to raise it encounters resistance from systems and payment models designed around the lower standard.
THE WRONG FIGHT
The preceding chapters documented the transport-only reimbursement model as a structural pathology—and it is. But the pathology is more precise than the profession has recognized. The problem is not simply that CMS pays too little. The problem is that CMS is being asked to fund something it was never designed to fund. The transport-only classification is the symptom. The absence of a readiness funding architecture is the disease. What follows reframes the CMS debate accordingly.
There is a deeper problem with the profession’s long campaign against CMS, and it is not that the campaign is unjustified. It is that it is probably misdirected. The grievance is real. But the target is wrong, and I fear this error has cost the profession decades of misallocated political energy.
Consider what an ambulance service actually spends its money on. The cost structure of any EMS agency divides into two fundamentally different categories. The first is readiness: the cost of having a staffed, equipped ambulance available to respond at any hour of any day, whether it is called or not—personnel, vehicles, equipment, facilities, dispatch, training, insurance, medical direction, and overhead. The second is the variable cost of an individual patient encounter: the consumable supplies used, medications administered, fuel burned on that specific response, and the clinician’s time in direct patient care.
A note on that last item, because a careful reader will object. EMS clinicians are typically salaried or paid by the hour, not by the call. Their wages are committed when the shift begins, regardless of patient volume. By strict accounting, crew compensation is a fixed cost—part of readiness. But this conflation of availability with service is itself a product of the broken model this section describes. In hospital settings, the same economic reality exists for most clinical staff. Nurses and respiratory therapists are salaried. Their time at the bedside is not billed as a separate professional fee. But their labor costs are covered—absorbed into the facility fee that Medicare pays the hospital on top of the physician’s professional charge. The facility fee exists precisely to fund the institutional cost of maintaining trained clinical staff around the clock, whether the census is full or the beds are empty. Physicians and advanced practice providers operate under a different model: they generate encounter-level professional fees billed directly to the patient’s insurer. The physician’s salary is an institutional cost; the physician’s clinical encounter is a billable event. EMS has access to neither mechanism. There is no facility fee to absorb the cost of having paramedics staffed and ready. There is no professional fee framework to bill for the clinician’s assessment, judgment, and intervention at the bedside. There is only a flat transport charge—a single payment that attempts to fund everything and inevitably funds nothing adequately.77
The ratio between readiness and variable costs is not close. Independent cost analyses across multiple states and service models consistently show that readiness accounts for approximately eighty to eighty-five percent of total EMS expenditures.75 The variable cost of an individual patient encounter represents fifteen to twenty percent. The overwhelming majority of every dollar an EMS agency spends is committed before the first call of the day is dispatched.
Now examine what Medicare actually pays. The ambulance fee schedule reimburses roughly three hundred to five hundred and fifty dollars for a BLS transport and five hundred to eight hundred dollars or more for ALS, depending on service level, geography, and mileage.76 Set aside for a moment the classification grievance, the supplier-versus-provider debate, the transport-only model. Look only at the numbers. If variable costs represent fifteen to twenty percent of total expenditures, the gap between what CMS pays per transport and the actual variable cost of the encounter may be far smaller than the profession has assumed. In many cases, Medicare’s reimbursement approaches or covers the variable cost of the clinical service delivered.
What CMS is not paying for, and what no per-transport reimbursement rate can ever pay for, is the readiness infrastructure that made the response possible. The two paramedics who were sitting in the station at three in the morning waiting for the call. The ambulance that was purchased, insured, maintained, and equipped whether it ran twelve calls that shift or none. The dispatch center. The medical director on retainer. These costs exist in full whether the system transports ten patients or ten thousand.
The profession has spent decades fighting for a higher rate on the fifteen percent while ignoring the question of who funds the eighty-five.
This distinction reframes the entire CMS debate. And it raises an uncomfortable possibility the profession has been reluctant to confront: it may not be appropriate to expect CMS, private insurance companies, or individual patients to fund readiness at all.
CMS, and other government and private payors, are health insurance payers. Their function is to reimburse for services rendered to individual beneficiaries. That is what health insurance does. We do not ask Medicare to build fire stations, staff police departments, or maintain 911 dispatch centers. We do not ask any insurance payer to fund the existence of infrastructure that serves everyone. We ask insurance payers to reimburse for the specific service delivered to the specific patient. By that standard, CMS may be doing roughly what an insurance payer should do.
The analogy that clarifies the argument is the one this chapter has already drawn. When a homeowner encounters a burglar, no one bills the homeowner’s insurance for the cost of the police department. The police department exists because the community decided, long ago, that police protection is a public good funded from the tax base—not loaded onto the person whose home happened to be targeted. EMS readiness is the same category of public good: non-excludable, demand-uncertain, and essential whether any individual patient needs it on a given day or not.
The pattern of error becomes visible once stated plainly. EMS first loaded the full cost of readiness—the eighty-five percent—onto its patients: the person having a cardiac arrest, the mother in labor, the child who fell off a bicycle. These are not consumers choosing a service. They are people in crisis, and EMS billed them not just for the care they received but for the entire infrastructure that made the care possible. When patients could not bear that cost, the profession did not question the model. It simply escalated the same flawed invoice upward, demanding that CMS—the patient’s insurer—absorb the readiness cost through higher per-transport reimbursement. The invoice did not change. Only the addressee did.
But it is not a reimbursement crisis. It is a model crisis. And the proof is visible in every hospital in the country.
THE HOSPITAL PROOF
The hospital comparison is instructive precisely because hospitals face the same readiness problem—and solved it by never relying on patient billing to fund their infrastructure in the first place.
The Hill-Burton Act of 1946 provided over six billion dollars in federal grants and loans to more than 3,500 hospitals. Adjusted for healthcare-sector inflation, that figure exceeds one hundred billion in 2024 dollars. By 1975, the program had financed nearly one-third of all hospitals in the United States. As of 2020, thirty-five percent of hospital beds still operating in America had received Hill-Burton funding.78 The federal government did not ask Medicare to build America’s hospitals. It built them through dedicated infrastructure investment, directly, before a single patient was billed.
The timing matters for the argument of this book. The Hill-Burton program continued providing grants and loans through 1997. In 1981—the same year the Omnibus Budget Reconciliation Act eliminated dedicated federal EMS funding, collapsed the regional EMS system architecture, and left state EMS offices to compete for diminished block grants—hospitals continued to access Hill-Burton support, tax-exempt bond markets, and the growing facility fee structure that would sustain them for decades. The federal government did not abandon healthcare infrastructure funding in 1981. It abandoned EMS infrastructure funding. Hospitals kept their architecture. EMS never had one to keep.
When Hill-Burton wound down, hospitals turned to tax-exempt bond markets—another public subsidy, since the tax exemption costs the federal government revenue. By the early 1980s, debt financed seventy-six percent of hospital construction.79 Today, tax-exempt bonds remain the single largest source of capital for hospital infrastructure. State and local governments contribute further: public hospitals are funded directly from the tax base, with county governments devoting twenty-one percent of their budgets to health and hospitals. Healthcare philanthropy added fifty-six billion dollars nationally in 2023. Hospitals also benefit from property and income tax exemptions—yet another public subsidy that EMS agencies rarely enjoy.80
And even with all of these mechanisms—federal construction grants, tax-exempt bonds, state and local appropriations, billions in philanthropy, and broad tax exemptions—hospitals still cannot fund their readiness costs through patient billing alone. That is why the hospital facility fee exists. The American Hospital Association describes facility fees as the mechanism that funds twenty-four-hour readiness: around-the-clock nursing, emergency and trauma capability, medical equipment, and critical infrastructure. In a 2024 survey by the Texas Hospital Association, eighty-five percent of hospitals reported they would need to reduce staff and eighty percent would cut services without facility fee revenue.81 The facility fee is, by the hospital industry’s own admission, a readiness subsidy—and even that is not enough without the other funding mechanisms standing behind it.
The facility fee is the strongest counterargument to the position advanced here. Medicare does pay hospitals a facility component that partially offsets readiness costs, and EMS advocates could reasonably argue that an equivalent mechanism is warranted. The argument has merit. But even hospitals do not fund their infrastructure primarily through CMS reimbursement. The facility fee is a supplement, not a substitute, and it evolved within a regulatory framework—accreditation, conditions of participation, provider classification—that EMS has never been granted. The facility fee argument supports seeking a readiness supplement from CMS. It does not support the expectation that CMS should be the primary funder of national EMS readiness.
Now consider EMS. No Hill-Burton equivalent has ever existed for ambulance services. No systematic access to tax-exempt bond markets. No philanthropic infrastructure. No broad tax exemptions. No facility fee. EMS has none of the readiness funding mechanisms that hospitals have used for eighty years—and the profession’s primary strategy has been to demand that CMS, the one source whose reimbursement may already approach the variable cost of the patient encounter, somehow cover everything. Hospitals, with five distinct readiness funding mechanisms, still cannot make patient billing cover their infrastructure costs. The notion that EMS, with zero such mechanisms, can accomplish what hospitals cannot through per-transport reimbursement alone is an illusion that has persisted for half a century because no one stopped to examine the arithmetic.
If EMS intends to operate as a healthcare profession—and this book has argued that it must—then the financial model must reflect how healthcare actually funds itself. The answer demands exactly two things: fund readiness as a public good, and bill patients and insurers for the fractional variable cost of the clinical encounter. Under that model, the per-transport reimbursement rates that CMS already pays may prove closer to adequate than the profession has recognized, because they would no longer be asked to carry the impossible weight of readiness costs they were never designed to cover. The full implications of this reframing are the subject of the final chapter. But the outline is already visible from here.
The rural crisis proves the point most forcefully. A volunteer ambulance service in a county that runs three hundred calls a year will never be financially sustainable on per-transport billing, regardless of how generous the reimbursement rate becomes, because there are not enough transports to amortize the readiness costs. Triple the Medicare rate tomorrow, and South Dakota’s ambulance services still cannot break even, because the problem was never the rate. The problem is that readiness costs eighty-five cents of every dollar, and no per-transaction billing model can fund a public good that exists whether or not the transaction occurs.
CMS is not the villain of this story. The absence of a readiness funding architecture is.
The profession’s frustration with CMS is understandable. It is not irrational. But it has become, over decades, a convenient misdirection—a way to externalize a political failure that is, at its root, a failure of the profession and the communities it serves to demand that EMS readiness be funded the way every other essential public safety function in America is funded. CMS is not the villain of this story. The absence of a readiness funding architecture is. And that absence will persist as long as the profession keeps sending its lobbyists to Baltimore when the fight that matters is in the state capitol and the county courthouse.
There is a simpler test of whether EMS is integrated into the American healthcare system, one that requires no finance or policy expertise to evaluate. Open the health app on your phone. If you visit your family physician, the clinical notes, vital signs, lab results, and diagnostic imaging are available to you, often within hours, through a patient portal you can access from your couch. If your physician refers you to a specialist, that specialist can see your records. If the specialist orders physical therapy, the therapist can see the referral, the imaging, and the clinical rationale. If the lab draws blood, the results populate across every provider in the network. And importantly, you, the patient, now have full transparency and access to your own clinical record. This is not cutting-edge innovation. It is the baseline expectation of modern healthcare delivery.
Now call 911.
In most EMS systems in the United States, a patient who has an ambulance system encounter will receive exactly one artifact from that experience: a bill. Not the twelve-lead ECG that the paramedic interpreted in the field. Not the vital signs trending during transport. Not the blood glucose reading, the medication administration record, or the clinical impression that guided treatment decisions. The patient cannot see their own chart. In many systems, the receiving hospital cannot efficiently access it either. The data that EMS generates in what is often the most acute, most consequential clinical encounter in a patient's continuum of care frequently vanishes into a system that is not connected to anything else.
Consider the patient who calls 911 with chest pain. A paramedic responds, obtains a twelve-lead ECG, checks a blood glucose, establishes IV access, administers aspirin and nitroglycerin, and monitors vital signs during transport. The clinical encounter is real, the interventions are real, and the data generated is diagnostically meaningful. The patient arrives at the emergency department. . . and, in most emergency departments in the United States, the first thing the receiving team does is repeat the blood glucose, obtain their own ECG, and start the diagnostic workup from scratch.
Why?
Is it because the hospital does not trust the paramedic's results?
Is it because the field data is not considered diagnostically sufficient?
Is it because there is no mechanism to transmit the information?
Whatever the reason, and in most cases it is some combination of all three, the result is the same: the clinical work performed by EMS is treated as provisional, something to be verified rather than built upon. That is not the behavior of an integrated healthcare system. It is the residue of a transport-centric model in which the ambulance delivers a patient, not a clinical record. EMS, as currently positioned in most of the country, functions as quasi-healthcare: close enough to medicine to perform clinical interventions, but not integrated enough for those interventions to follow the patient through the door.
To be fair, isolated exceptions exist. Some progressive EMS systems have built direct data integration with their receiving hospitals, and a handful of regions have achieved meaningful interoperability between prehospital and hospital electronic health records. These examples deserve recognition and study. But they remain exactly that: exceptions, achieved through local initiative rather than systemic architecture. The more common reality is that EMS agencies have found ways to eventually transmit data to hospitals, not for clinical integration, but for compliance. Systems are still faxing patient care reports or transmitting PDF attachments, documents that are essentially useless in the era of structured electronic health records because they cannot be parsed, queried, or incorporated into a patient's longitudinal medical record. The data arrives, technically, but it arrives dead on arrival.
The irony is that EMS is simultaneously home to one of the most powerful electronic health record infrastructures in American healthcare. The National EMS Information System, NEMSIS, collects over sixty million patient care records annually in near real time, an extraordinary repository of clinical, operational, and epidemiological data with immense value for research, public health surveillance, and national security planning. But that infrastructure, for all its scale, is not interconnected with hospital systems, is not accessible to the providers who receive EMS patients, and is not transparent to the patients whose encounters it documents. EMS has built a national data system of remarkable scope and then walled it off from the healthcare ecosystem it was meant to serve.
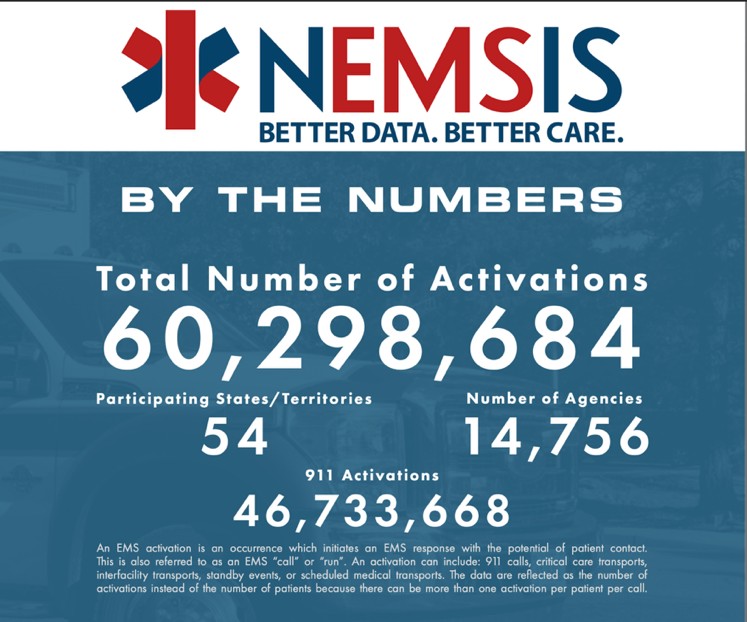
Every other healthcare discipline has resolved this. Primary care, specialty medicine, laboratory services, radiology, pharmacy, physical therapy, behavioral health: all have been drawn into interoperable health information ecosystems (at least locally or in certain networks) where data flows between providers and patients have access to their own records. EMS, for the most part, remains outside that ecosystem. Clinical data that is neither shared with the providers who need it nor visible to the patients who own it. This is not a technology problem. The technology exists and has existed for years. Electronic patient care reporting systems are capable of interoperability. Health information exchanges can accept EMS data. The barrier is predominately structural and cultural: EMS was built as a transport system, reimbursed as a transport system, and its data infrastructure reflects that origin. A transport system does not need to share clinical records, because a transport system does not generate clinical care. But EMS does generate clinical care, and until its information systems reflect that reality, the profession's claim to clinical parity will remain exactly that: a claim, unsupported by the most basic infrastructure that every other medical discipline takes for granted. If EMS intends to be recognized as a medical profession by its peers, its patients, and its payers, this is among the most urgent gaps to close. The profession cannot demand a seat at the healthcare table while remaining invisible in the healthcare record.
The “essential service” paradox is the clearest expression of this legacy. EMS functions as essential everywhere in the country. No community in America would voluntarily go without ambulance service. But state after state cannot bring itself to designate EMS as legally essential, because doing so would require funding it—and the funding architecture does not exist. The designation without the funding would be hollow, as Senator Reed correctly recognized. But the absence of the funding architecture is precisely what the Dark Age bequeathed. Consider: in 1862, Surgeon General William Hammond urged Congress to establish “a permanent hospital and ambulance corps, composed of men specially enlisted for duty in the Medical Department.” Congress acted—then let the system expire when the Civil War ended. In 1885, Surgeon General Robert Murray renewed the call. Congress responded with the Hospital Corps Act of 1887. Colonel Charles H. Alden, placed in charge of that Corps and first president of the Army Medical School, spent the 1890s building the institutional architecture Hammond had envisioned three decades earlier. More than 160 years after Hammond’s original plea, the civilian nation still does not have a permanent, structured emergency medical system.
In 1862, Surgeon General Hammond asked Congress for a permanent hospital and ambulance corps. More than 160 years later, America still does not have one.
The question is why, in 2026, the richest nation in history still has no financial architecture for emergency medical services while multiple developing nations around the globe have implemented ‘world-class’ sustainable solutions.
The question is not rhetorical. While the United States was encoding the Dark Age’s transport-only model into Medicare reimbursement, other nations were building the financial architecture America never did. The following table is not exhaustive, but it illustrates a point: publicly funded, nationally recognized emergency medical services are not a policy fantasy. They are operational realities across multiple continents, economic systems, and governmental structures.
The question is why, in 2026, the richest nation in history still has no financial architecture for emergency medical services.
Table: Selected international examples of funded national EMS systems. This list is illustrative, not exhaustive.
Sustainable, national EMS systems that are funded are not theoretical. They exist, they function, and they span the full range of economic development and governmental structure. The United States built the original model. American physicians designed the physician-staffed ambulance, American cities funded it as a core municipal service, and American military medicine exported the concept to Europe through two world wars. Other nations took that foundation and improved upon it. Both prosperous economies and developing nations have reached the same conclusion: emergency medical services are essential to national security, public health, and healthcare delivery, and essential services require dedicated, sustainable funding.
Sri Lanka, a nation with a fraction of America's GDP, operates a nationally funded ambulance system with standardized training, centralized dispatch, and universal coverage. The question facing the United States in 2026 is not whether a funded national EMS architecture is possible. A dozen countries on this list have already answered that question. The question is why the nation that invented the concept is now the outlier that has failed to sustain it.
If the Dark Ages parallel holds, then the historical pattern suggests that certain developments may represent the first genuine emergence from prolonged stagnation.
The growth of community paramedicine and mobile integrated healthcare represents the most structurally significant shift: EMS returning to its original clinical identity—treating patients, providing out-of-hospital medicine, and only transporting them if clinically indicated. When a community paramedic manages a chronic disease patient at home and prevents a hospital admission, the ambulance is no longer functioning as a taxi to the emergency department. It is functioning as a clinical resource deployed where it is needed. This is closer, in principle, to the physician-staffed ambulance of the 1880s than to the hearse of the 1950s. But community paramedicine, as currently implemented, largely operates within the existing reimbursement framework rather than replacing it. Medicare’s ET3 pilot program—which tested payment for treat-in-place and alternative destination transport—was a step toward aligning payment with clinical reality, but it remained a pilot, not a permanent structural reform. The clinical model is evolving. The payment model is experimenting.
Interstate licensure portability, now operational through the EMS Compact across twenty-five states, addresses a different layer of the Dark Age’s legacy: the workforce fragmentation caused by fifty separate state systems that could not share personnel across borders. The Compact does not solve the funding crisis directly, but it removes a structural barrier that the 1966–1973 federal fragmentation helped create—the assumption that EMS is a purely local concern, organized state by state, with no national coherence.
Technology integration—artificial intelligence, telemedicine, advanced prehospital diagnostics—is also expanding what field providers can do, but capability without reimbursement is aspiration without architecture. A paramedic who can initiate a blood transfusion, perform an ultrasound, or interpret a twelve-lead ECG without transmitting it to a cardiologist is practicing at a level the profession’s founders would recognize as genuinely advanced. Whether that paramedic is paid accordingly is a different question, and the answer, in most systems, is no.
But the deeper question may not be whether these incremental advances can fix the existing architecture. It may be whether the existing architecture is about to be rendered obsolete. In 1899, when Michael Reese Hospital deployed Chicago’s first motorized ambulance, the transition from horse-drawn to motor-powered vehicles was not a marginal improvement—it was a categorical leap. By 1903, Hartford (CT) reported that motor ambulances cost fifty percent less to operate, were instantly ready, and each replaced five horses. Within a decade, the horse-drawn ambulance was functionally extinct. Today, EMS may be approaching a convergence of similar magnitude. Vertical takeoff and landing aircraft are being developed and tested for emergency medical transport—overcoming the geographic barriers that have defined rural EMS since the profession’s founding. Autonomous vehicle technology is advancing toward a future in which the staffing crisis that is hollowing out services like South Dakota’s may be addressed not by lowering training standards but by changing the nature of the vehicle itself. And artificial intelligence decision support is expanding the clinical reach of every provider in the field—not replacing the paramedic, but extending the paramedic’s diagnostic and treatment capability in ways that begin to close the gap between prehospital and hospital-based care. Any one of these developments, taken alone, would represent a significant disruption. Their simultaneous convergence suggests something closer to a phase transition—not an upgrade to the existing system, but a redefinition of what the system is. The question for EMS leaders is whether the profession will build toward that future or continue optimizing within an architecture that may not survive it.
Air medical transport has been a reality since the helicopter evacuations of Korea and Vietnam, and rotor-wing EMS has operated in the United States for half a century. But advanced air mobility—urban VTOL aircraft, autonomous drone delivery of blood products and AEDs to cardiac arrest scenes—represents something categorically different: not faster helicopters, but a redefinition of what “transport” means when geography is no longer a constraint.
The skepticism from experienced clinicians is predictable and, within its own frame, reasonable. No flight nurse or critical care paramedic is eager to board an autonomous electric aircraft without a pilot. Helicopter EMS exists, works, and has decades of operational refinement behind it. Why chase an unproven technology when a proven one is already flying? But this objection assumes the disruption looks like the current model with a different airframe. It may not. A drone delivering packed red blood cells to a rural trauma scene does not require a crew aboard—but it requires a crew on the ground ready to receive the delivery. An autonomous aircraft meeting EMS clinicians at the scene does not replace the EMT or Paramedic. It provides an alternative that, if current estimates hold, will be safer, less expensive, faster, and more widely deployable. The disruption is not asking clinicians to fly on machines they do not trust. It is asking whether the missions we currently cannot serve—because helicopters cost thousands of dollars per flight hour and reach only a fraction of EMS calls—might be served by something that changes the economics entirely.
In 1899, the skeptics were right that horses were more reliable than early motor vehicles. They were wrong about what that fact meant for the future. The question was never whether the first automobiles were better than horses. The question was whether the trajectory of the technology would eventually make the comparison irrelevant.
Whether these developments represent the opening act of a genuine renaissance or merely incremental improvements within the same compromised framework depends on a single question: will the nation finally build the financial and political architecture to support what its EMS clinicians can already do? Community paramedicine, interstate portability, and advanced technology are each genuine achievements. But achievements built on top of the Dark Age’s broken foundation remain vulnerable to the same forces that destroyed the systems of the 1930s. A renaissance is not a renaissance until the floor is replaced, not merely decorated.

A renaissance is not a renaissance until the floor is replaced, not merely decorated.
Chapter 7 — The Broken Promise
The preceding chapters explored the external forces that shaped American EMS: the wars that stripped physicians from American ambulances, the economic collapses that gutted municipal budgets, the funeral industry that filled the vacuum with hearses, the federal compromises that encoded transport-only reimbursement into permanent policy. These were forces imposed upon a profession that had little power to resist them. The argument, as presented so far, casts EMS as the object of history. In some ways, the victim of circumstance, the evolution of American EMS was something that history happened to.
I believe this framing is appropriate and accurate for the period between 1930 and 1966. However, it is incomplete for 2026.
In 2026, the most consequential resistance to the professionalization and advancement of emergency medical services is no longer exclusively external. It is also internal. Segments of the profession itself—our clinicians, our institutional leadership, our cultural identity—have become significant barriers to the very reforms that can elevate EMS from its current marginal status. At some point, a profession must stop asking to be recognized as something and start consistently acting like it. Now, I recognize that this is not a comfortable argument, and it is not offered lightly. But the evidence is now sufficient that intellectual honesty demands its examination.
This resistance is rarely malicious and is often rooted in legitimate fears about workforce sustainability, rural access, and system survival. However, when these concerns consistently translate into opposition to education, accountability, and clinical integration, the long-term effect is professional stagnation regardless of intent.
At some point, a profession must stop asking to be recognized as something and start consistently acting like it.
Understanding why segments of the EMS profession resist national structure requires understanding what happened the last time the profession trusted it.
In the 1970s, the federal government made an extraordinary commitment to Emergency Medical Services. The Emergency Medical Services Systems Act of 1973 funded the development of three hundred regional EMS systems across the United States. Federal dollars flowed to states. Regional systems were designed, staffed, and launched. State EMS offices were established, many for the first time, with dedicated federal support. Medical directors were appointed. Training programs were built. Communications systems were funded. For a brief, remarkable period, EMS had what it had never had before: a national plan, national funding, and national momentum. The promise was explicit. The federal government would build the architecture, fund the development, and then transition the systems to state and local sustainability over a defined period.
Then, in 1981, the Omnibus Budget Reconciliation Act collapsed the entire structure virtually overnight. Dedicated EMS funding was consolidated into state-administered block grants, where it competed with dozens of other health and social programs for a share of diminished allocations. The designated lead federal agency for EMS within the Department of Health and Human Services was eliminated. Most provisions of the 1973 Act were repealed. Of the three hundred planned regional EMS systems, roughly forty percent were still in active development, but all of them were defunded mid-construction. A 1986 General Accounting Office analysis of six states found that EMS expenditures had fallen below 1981 levels by 1985. State EMS offices that had existed for less than a decade lost their federal mandate, federal funding, their federal guidance, and in many cases their staff. The generation of EMS leaders who had built their systems on the promise of sustained federal support were left holding an empty basket.
1970's Map of the EMS Regions for Massachusetts. Similar maps were created for each state under the original EMS Systems Act.
Contemporary accounts confirm the scale of the devastation. A 1982 survey published in Hospitals magazine found that of the 303 EMS regions designated between 1974 and 1981, only fifty-seven—nineteen percent—had completed their five-year development cycles before categorical funding was eliminated.73 The HHS Division of Emergency Medical Services, the agency that had directed the federal effort for eight years, was reduced to three staff members awaiting the office’s extinction. R. Adams Cowley, the trauma care pioneer who directed Maryland’s EMS program, estimated that the nation was only “about a third of the way” toward an effective nationwide system—after eight years of dedicated federal investment and $309 million in categorical spending. The states, for their part, had not been idle. The Department of Transportation reported that federal and state government spending combined accounted for only ten to twenty-two percent of what was actually being spent on EMS, meaning that local governments and communities were investing far more of their own resources than the federal contribution required. The commitment was real. But a 1976 report by the Comptroller General had already warned Congress that the structural conflict between the Department of Health, Education, and Welfare and the Department of Transportation—with over thirty uncoordinated federal programs touching EMS and an Interagency Committee that took more than a year to begin functioning—was undermining the very regional systems those local dollars were trying to build.74 The federal government had not merely failed to sustain its promise. It had failed to organize its own effort coherently while the promise was still being made.
The consequences were immediate and lasting. Without unified federal standards or dedicated funding, states diverged rapidly. Each developed its own certification levels, training requirements, and examination standards. By the 1990s, the United States had more than forty documented variations of EMT certification, a fragmentation so severe that EMS professionals often could not transfer credentials across a state line. The national coherence that the 1973 Act had promised, and that the profession had organized itself around, simply evaporated.
But here is what matters most for the argument of this chapter. The generation that lived through the 1981 collapse developed a deep, rational, and entirely justified resentment toward national and federal structure. These were not ideologues opposed to standards on principle. These were people who had trusted the federal government, built systems on that trust, watched the government walk away, and then had to scrape together local solutions from whatever was left. They built village, town, and county EMS systems through personal sacrifice, local fundraising, and sheer determination. Those systems did not always meet the national standards that had been abandoned, but the national standards had failed them first. The resentment was earned.
The problem is what happened next. That resentment was transmitted to the next generation. And the next. Over decades, the institutional memory of betrayal became an institutional reflex of resistance, passed down through mentorship, through organizational culture, through the accumulated weight of "that's not how we do things here." The newer generations inherited the resistance without inheriting the rationale. They knew that their mentors distrusted national standards, federal coordination, and centralized credentialing. They absorbed that distrust as professional identity. But many never learned why the distrust existed in the first place, because the story of the broken promise was not taught. It was simply felt.
The parallel to the Hatfield-McCoy feud is uncomfortably precise. After enough generations, the participants no longer remember the original grievance. They simply know that resistance is what they do. It is part of who they are. And anyone who questions it is treated not as a reformer but as an outsider who does not understand.
I understand the grievance. I have worked in systems that were built from the wreckage of the 1981 collapse, by people who had every reason to distrust promises from Washington. Their skepticism was not irrational. It was survival. But survival strategies have a shelf life. The federal government that broke its promise in 1981 is not the same institutional landscape that exists in 2026. The EMS Compact, the National EMS Education Standards, the accreditation infrastructure, the interstate credentialing framework: these were not imposed by a distant federal authority. They were built by the profession itself, by state EMS directors, by educators, by medical directors, by the same kinds of local leaders who rebuilt after the collapse. Resisting these structures because of what happened forty-five years ago is not protecting the profession. It is punishing the present for the sins of the past.
The broken promise of 1981 explains the resistance. It does not justify its perpetuation.
Every EMS professional who entered this field after 1981 inherited a system shaped by a betrayal they never experienced. The question is whether they will build anything better.
The inherited resistance to national structure found its most visible and enduring target in the National Registry of Emergency Medical Technicians (NREMT).
The NREMT was established in 1970 as a direct product of the same federal initiative that created the modern EMT. President Lyndon Johnson's Committee on Highway Traffic Safety formed a task force, led by the American Medical Association, to establish a national EMS certification agency. The task force included representatives from the Ambulance Association of America, the International Association of Fire Chiefs, the National Funeral Directors Association, the National Safety Council, the American Heart Association, and others. On June 4, 1970, the first meeting of the Board of Directors of the of Emergency Medical Technicians was convened.
The new organization (and new profession) needed a symbol. What it received was far more than a graphic design. The American Medical Association in 1970 was not merely a professional association. It was the most powerful institutional authority in global medicine, the gatekeeper of who could practice, what could be taught, and which professions would be recognized as legitimate within the medical establishment. The AMA had already branded its Universal Medical Identification Symbol worldwide, securing its adoption by the World Medical Association in Helsinki in 1964 and its recognition by the FBI, the Department of Transportation, and international health agencies. The symbol carried the full institutional weight of organized medicine.
The AMA was doing something unprecedented with EMS. It was creating an entirely new category of medical professional: non-physicians who would start intravenous lines, intubate airways, interpret cardiac rhythms, and administer medications in the field. This was a scope of practice and clinical autonomy that simply did not exist outside of physician practice. The resistance from within healthcare was real. Nursing organizations and allied health professions questioned why ambulance personnel should be permitted to perform procedures that their own practitioners had fought for decades to secure. The AMA overrode those objections. It created the EMT-Basic, and then recognized the EMT-Paramedic through the same allied health accreditation pathway it controlled. The AMA staked its brand and institutional credibility on the legitimacy of this new profession.

When the AMA transferred its symbol to the Registry of EMTs, it was not donating a logo or a graphic design. It was conferring institutional protection. In medieval terms, it was the king providing a letter of safe passage to a traveler: interfere with the bearer, and you answer to the crown. The Star of Life on an EMT's patch meant that this provider, and this profession, operated under the explicit endorsement and authority of the most powerful body of organized medicine on the planet: the American Medical Association.
In 1971, the first 1,520 ambulance personnel took the first standardized national EMS certification examination at fifty-one testing locations across the United States. The successful candidates received a patch bearing that symbol: a direct connection to the brand, the authority, and the institutional protection of the most powerful medical organization in the world, signifying both demonstrated competence and adherence to a unified national standard.
When the 1981 collapse fragmented the national EMS architecture, the NREMT became collateral damage. States that lost federal funding and federal guidance began developing their own certification examinations, their own training requirements, and their own provider levels. Many of these state-specific systems were built not because the national standard was inadequate, but because the states could no longer afford or access the infrastructure that supported it. The divergence was, in many cases, a forced adaptation to abandonment. But over time, the adaptation hardened into preference, and the preference hardened into identity. States that had created their own examinations developed institutional ownership of those examinations. The state exam became a point of pride, a marker of local sovereignty, an assertion that we know our own needs better than any national body.
Since that fragmentation, the arguments against the NREMT examination have remained remarkably consistent over four decades: the exam is too hard, it does not reflect local protocols, it creates barriers to entry in an understaffed profession, and states have the sovereign right to determine their own standards. Each argument contains a grain of truth wrapped in a larger evasion. The examination is rigorous, as any national medical licensing examination should be. It does not test local protocols, because a national standard by definition cannot be local. It does create a threshold, because thresholds are what distinguish professions from occupations. And states absolutely possess the sovereign right to determine their own practice standards, a right that is not in dispute and never has been.
Now, a disclosure. I was employed by the National Registry of EMTs for five years, and served as its Chief Operating Officer. I am not a disinterested observer on this subject, and the reader should weigh my perspective accordingly. I would not argue that the NREMT is a perfect organization. No institution is. But I will argue, from direct experience and from the evidence, that the fundamental design of the national certification examination is sound.
The examination is passed by thousands of candidates every year. It is psychometrically validated, legally defensible, and aligned with the National EMS Education Standards. In 2024 alone, over 150,000 candidates sat for NREMT certification examinations across all provider levels. Seventy-nine percent of paramedic candidates passed. Seventy-four percent of EMT candidates passed. These are the pass rates of an examination that the majority of adequately prepared candidates clear on the first attempt. When pass rates are low, the pattern is consistent and well-documented: low first-time pass rates correlate with local educational program characteristics, not examination design.
The data bears this out at the state level. In 2024, first-time paramedic pass rates ranged from 65% to 100% across all fifty states. Every paramedic program is accredited through CoAEMSP. All of their instructors hold national certification. All of their graduates sat for the same examination. The variation that remains is not attributable to accreditation status, instructor credentialing, or examination design. It is attributable to program quality, and this is the one variable the profession has consistently refused to make visible.
The EMT data tells the same story from the opposite direction. EMT programs, which carry no independent programmatic accreditation requirement, produced a thirty-two-point spread in cumulative pass rates over the same period. The states that cluster at the bottom of the paramedic list are largely the same states that cluster at the bottom of the EMT list. Accreditation raised the floor and paramedic programs generally outperform EMT programs. The lowest-performing paramedic states outperform the lowest-performing EMT states. That is genuine, measurable progress, and CoAEMSP deserves credit for it. But accreditation was designed to establish structural minimums, not to guarantee outcomes. It was never intended to be the sole mechanism of accountability, and treating it as such places a burden on accreditation that accreditation cannot bear.
The NREMT publishes current pass rate data by state at nremt.org/maps. I encourage you to look. Find your state. Compare it to your neighbors. The NREMT also provides program-level pass rate data directly to every state EMS office in the country. The decision to publish that data — or to keep it hidden — belongs to each state. In my experience as a state EMS director, one of the most profound political pushbacks I faced was attempting to publish this data. Powerful stakeholder groups inside EMS rallied against me for trying. The resistance was not about data quality or methodology. It was about exposure, and exposure would have revealed what every EMS professional already knows but few are willing to say publicly.
Every EMS professional knows “Bob”.
Bob is the experienced provider who ended up teaching because he was injured and placed on light duty, or because he was the senior guy who had been around the longest, or because he volunteered and nobody else stepped up. Bob may be passionate. He may be a good clinician. But Bob's classroom runs on war stories and anecdotes. The textbook says one thing; Bob tells you how it really works on the street. Bob's students may enjoy the class. They are not being prepared for a national certification examination, and they are not receiving the foundational medical education that a career in emergency medicine demands. Bob runs an EMT class every year and has a twenty percent first-time pass rate, and Bob will tell you it is because the exam is broken.
It is far easier to blame an impersonal national examination than to hold a local program accountable, or to confront the reality that Bob, the local instructor you know and respect, is not qualified to teach a medical profession. But directing anger at the exam rather than at the program that failed to prepare you allows the core problem to persist unchallenged, producing the next class of underprepared candidates while changing nothing.
This is not Bob's fault. Bob was placed in a role the system should never have asked him to fill without ensuring he had the pedagogical training, institutional support, and educational resources to do it well. The failure belongs to the programs and regulatory structures that allow unqualified instruction to continue without consequence, not to the individuals who stepped into a vacuum no one else was filling.
I believe there is a straightforward remedy that would address the majority of these issues without requiring a single new regulation: data transparency.
Every state EMS office already receives program-level data from the NREMT. They know which programs produced how many candidates, how many passed on the first attempt, and how many passed by the third attempt. The information exists. It is simply not published in most states. A 2022 study published in Prehospital Emergency Care64 confirmed what the data suggests: program performance on the national certification examination varies significantly by program size and geographic region, with the smallest programs producing the lowest pass rates and wide regional disparities that persist across both EMT and paramedic levels.
Then ask the harder question: why is this data available at the state level but not the program level?
Georgia, in my opinion, has the most transparent EMS education program data available nationally. Georgia publishes program-level EMS education pass rate data on a public dashboard, ranking every program in the state by examination performance — including enrollment, completion, attrition, and pass rates at every certification level, updated on rolling three-year windows. A prospective paramedic student in Georgia can compare a program with a 96% first-attempt pass rate against one with a 17% first-attempt pass rate before investing a single dollar. Utah also publishes three-year cumulative pass rates for every EMS education program in the state, sourced directly from the NREMT, explicitly stating that "access to this data is crucial for prospective students as they consider their training options." The infrastructure exists. The data exists. The precedent exists. What is missing is the will to make it universal.
All states should publish raw pass rate data from the NREMT for every EMS educational program, quarterly and annually: number of candidates, first-attempt pass rate, and cumulative pass rate by third attempt. Let the data speak. The public has a right to know whether the program training their community's paramedics is producing competent graduates or cycling students through a system that fails them. Prospective students investing thousands of dollars and months of their lives deserve to see the outcomes before they enroll. Programs that are chronically underperforming deserve to be visible, not shielded by the opacity that allows them to continue operating without consequence.
Will raw data occasionally look misleading in isolation? Of course. A program with two candidates and one failure shows a fifty percent pass rate. But the public is capable of reading context, and that number raises its own question: why is a program operating with two candidates? Transparency does not require perfection. It requires honesty. And honesty, in a profession that claims to be accountable, should not be controversial. Transparency of program performance data is the standard among our medical colleagues. I encourage you to test this claim: select any nursing school, medical school, or physician assistant program, and you can find their examination performance data published openly.
Now try to find the pass rates for the EMT and paramedic programs in your community. If you live in Georgia or Utah, you can. If you live in many states, you cannot.
This is not a failure of state EMS offices. Most state EMS directors I have worked with understand the value of transparency and would welcome it. The resistance comes from inside the EMS industry itself — from the programs, organizations, and stakeholder groups that benefit from opacity and have fought transparency at every turn. It is time for the profession to say, collectively and without equivocation: this is the national standard. Every EMS education program in every state should be required to publish primary source pass rate data, directly from the NREMT, accessible to every prospective student and every community that depends on these programs to produce competent providers. No exceptions. No delays. No excuses.
Regarding the national examination and state alternatives. No other healthcare profession tolerates this debate. Nursing has the NCLEX. Physician assistants have the PANCE. Respiratory therapists have the NBRC examination. In each case, a single national examination validates entry into the profession, administered after completion of an accredited program, with no state-by-state alternative. A nursing graduate in North Carolina takes the same examination as a nursing graduate in California. No state legislature has proposed creating an alternative state nursing exam because local pass rates were unsatisfactory. The very idea is absurd, and yet in EMS it is not only proposed but enshrined as a local badge of honor. North Carolina and New York maintain alternative state examinations to this day. Michigan, as documented in Chapter 8, has now legislated a third.
The fragmentation has been largely, though not entirely, resolved. In 2026, all states now recognize National EMS Certification as the pathway to state licensure, albeit North Carolina, New York and soon Michigan will also have their alternative path. That represents decades of painstaking, considered work by state EMS directors, the National Association of State EMS Officials (NASEMSO) , the NREMT, and countless individuals who understood that a profession cannot function as fifty separate professions. But the cultural resistance persists in pockets, sustained by inherited grievance, institutional inertia, and the understandable human tendency to blame the standard rather than the preparation.
To be clear: I am not questioning the knowledge or abilities of EMS clinicians in these states, and their education programs may well meet national education standards. That is not the issue. The issue is that state-specific licensure examinations, however rigorous, represent a fragmentation of the EMS profession at precisely the moment the profession most needs to speak with one voice. A profession that cannot unify around a common credentialing standard cannot credibly present itself as a unified national profession — and until it does, it will continue to undermine its own advocacy for the recognition and reform it seeks. The path forward is one most states have already walked: grandfather existing practitioners under their current credentials, allowing them to continue practicing until retirement. Simultaneously, transition new entrants to nationally recognized certification. The things within our control as a profession — and national credentialing unity is squarely within our control — must be addressed before we can expect the federal investment we seek.
I will share a moment that clarified this issue for me in a way that no data set ever could.
Early in my time at the National Registry, I sat across from a state EMS director — someone I respected, someone who dedicated their career to building a state's EMS system — and listened to him explain, with genuine conviction, why his state would never adopt the national certification examination. His arguments were familiar: the national exam didn't reflect some unique local protocols, his providers knew their communities better than any national standard could capture, and his state had been burned before by trusting federal promises. I understood every word. I had worked in systems built by people just like him, and I knew the betrayal he was describing wasn't theoretical. It was biographical.
But as the conversation continued, I began asking questions: did his state's examination meet the Standards for Educational and Psychological Testing — the joint standard published by the American Educational Research Association, the American Psychological Association, and the National Council on Measurement in Education that governs every defensible high-stakes examination in the country? It did not. Did the state employ PhD-qualified psychometricians to analyze the examination? Did anyone conduct item-level bias analysis to detect cultural drift or differential performance across demographic groups? Was every question monitored, consistently, to ensure validity? Did they track whether examination items had been publicly exposed and compromised? Had the state conducted a practice analysis — a systematic study of what paramedics actually do in the field — to ensure the examination reflected current clinical reality rather than the assumptions of whoever wrote the questions?
The answer, in each case, was no.
The NREMT examination does all of this. It meets the Standards for Educational and Psychological Testing, and that is the same evidentiary framework that has been upheld by the United States Supreme Court as the benchmark for defensible professional credentialing examinations. Every item is written, reviewed, and statistically analyzed by qualified psychometricians. Every question is monitored for bias, validity, and exposure. The examination content is anchored to a national practice analysis conducted on a recurring cycle, ensuring that what the exam tests is what paramedics actually do. This is not a bureaucratic exercise. It is the scientific infrastructure that separates a credentialing examination from a quiz.
And that was the moment the argument shifted for me — not against him, but past him. His resistance was rational. It was historically grounded. But his state was defending an examination that could not survive the legal and scientific scrutiny that the national examination was specifically built to withstand. The energy his office spent maintaining that instrument was energy not spent on program oversight, system development, or the workforce crisis consuming his rural counties. He was fighting yesterday's war with resources his state could not afford to spend.
My blunt assessment is this: the EMS profession has to move on. We have a national standard grounded in solid science. The examination is legally defensible and passed by the overwhelming majority of adequately prepared candidates. Continued resistance is not a policy debate — it is a resource drain, consuming time, effort, and legislative influence that should be directed at fights that actually matter.
What remains is the echo of a broken promise from 1981, reverberating through a profession that has not yet reckoned with the difference between justified historical grievance and self-defeating institutional habit. And as Chapter 8 documents, the problem is no longer merely inherited — it is being actively recreated.
The argument that educational mandates and credentialing reform will destroy the EMS workforce is not a novel claim. It is the same argument that was advanced against similar reforms in pharmacy, nursing, and respiratory therapy. In each case, the predicted catastrophe did not materialize. In each case, the reforms produced the professional recognition and structural gains that EMS continues to lack.
Pharmacy is perhaps the most instructive example. Through the mid-twentieth century, pharmacists could practice with a bachelor's-level degree, and the profession functioned largely as a dispensing trade. The transition to the Doctor of Pharmacy (PharmD) as the sole entry-level credential was fiercely opposed by segments of the profession who argued that it would reduce the workforce, increase costs, and offer no measurable improvement in patient outcomes—arguments virtually identical to those now advanced against degree requirements in EMS. The PharmD mandate was implemented incrementally, with transition timelines that allowed existing practitioners to continue under their current credentials. The workforce did not collapse. The profession gained clinical prescribing authority, direct patient care roles, provider status recognition, and compensation parity with other doctoral-level healthcare disciplines. The credential became the floor on which the profession built its future.
Nursing's "BSN in 10" initiative demonstrates that phased transitions can raise educational floors without the workforce disruption that opponents predict. The campaign, now endorsed by multiple state legislatures and nursing organizations, requires newly licensed registered nurses to obtain a bachelor's degree within ten years of initial licensure. Existing practitioners are grandfathered. New entrants have a clear, achievable timeline. The model acknowledges that workforce constraints are real while refusing to accept them as permanent justification for lower standards. It is a strategy that treats the workforce shortage and the educational deficit as two problems requiring two solutions rather than using one as an excuse to ignore the other.
Respiratory therapy followed a similar trajectory: raising the credential floor from associate to baccalaureate level while maintaining workforce pipelines through transition provisions, grandfathering, and expanded training capacity. The profession experienced the temporary disruption that any structural change produces. It did not experience the existential collapse that was predicted. And the higher credentialing standard became the foundation for expanded scope of practice, greater professional autonomy, and higher compensation.
But the most instructive comparison is not pharmacy or nursing or respiratory therapy. It is the physician assistant.
It is worth noting where the PA profession began educationally, because the comparison is frequently dismissed on the assumption that PAs were always a graduate-level discipline. They were not. The first PA programs were certificate programs. Through the 1970s and 1980s, most PA graduates held associate degrees or certificates — credentials comparable in level and duration to paramedic training of the same era. A paramedic student in the 1980s choosing between a PA program and a paramedic program at the same community college faced two paths of roughly equal length and academic demand. One path led to a profession that would systematically raise its educational floor over the next three decades — from certificate to associate to bachelor's to master's — while building the accreditation infrastructure to make each transition stick. The other led to a profession that would hold its educational floor at the certificate or associate level for sixty years and treat any proposal to raise it as a threat to the workforce. The PA profession did not start above EMS. It started beside it. And then it climbed.
The PA profession was born in 1965 — the same decade as modern EMS, from the same workforce pool, in response to the same national crisis. Eugene Stead at Duke University assembled his first PA class from former Navy corpsmen, military-trained medical personnel whose clinical experience had no civilian credential to match it. The parallel to the military medics and corpsmen who became the first generation of paramedics is not approximate. It is exact. Both professions were created by physicians who recognized that military medical training had produced clinicians capable of far more than civilian healthcare systems allowed them to do. Both were backed by federal funding in the early 1970s. Both were intended to extend healthcare access to underserved communities. And both faced the same structural question every new profession faces: how do you build institutional coherence before the window of political support closes?
The PA profession answered that question in a single decade. The Physician Assistant History Society identifies four pillars of a profession: a society of practitioners, an association of educational programs, a nationally recognized accreditation body, and a process of certification in the public interest. By 1975, PAs had all four in place and functioning with paid executive management. The American Academy of Physician Assistants was established in 1968. The Association of Physician Assistant Programs followed in 1972. The AMA's Joint Review Committee (the same committee that approved the EMT-Paramedic profession) began accrediting PA programs that same year. The National Commission on Certification of Physician Assistants was formed in 1974, and the first national certifying examinations were administered through the National Board of Medical Examiners in 1973.63 When the NCCPA issued its first certificates in 1975, state medical boards immediately began recognizing them as qualifications for practice. The profession did not wait for fifty states to develop fifty different standards. It built one standard and made it authoritative.
EMS was not behind. Actually, it was ahead, briefly. The National Registry of Emergency Medical Technicians was established in 1970 by the AMA. This was before the NCCPA existed. The EMS Systems Act of 1973 provided federal funding for regional EMS systems, just as the Comprehensive Health Manpower Training Act of 1971 funded PA education. For a few years in the early 1970s, both professions were on parallel tracks, building national infrastructure with federal support.
Then the tracks diverged. When the Omnibus Budget Reconciliation Act of 1981 consolidated federal health funding into block grants, the PA profession's education pipeline survived. Title VII, Section 747 of the Public Health Service Act preserved dedicated federal funding for PA programs, and this funding remains in place today. EMS lost everything. The lead federal agency was eliminated. The regional systems were defunded. The national architecture was abandoned. But here is the critical difference: the PA profession had already built its internal infrastructure — the accreditation body, the certifying commission, the professional society, the educational standards — before the federal withdrawal. When Washington stepped back, the profession stood on its own pillars. EMS had not finished building its pillars. When Washington stepped back, the structure collapsed.
What followed was a half-century divergence. PAs maintained a single national accreditation body and national certifying examination. EMS allowed states to opt out of the National Registry, create alternative examinations, and fragment the credentialing system into dozens of state-specific variations. PAs required their educational programs to meet nationally accredited standards from the beginning. EMS allowed program quality to vary so widely that a paramedic trained in one state might not meet the entry standards of the state next door. PAs achieved prescriptive authority in all fifty states by 2007. Paramedics cannot prescribe medications they are authorized to administer. PAs were named in the Affordable Care Act as one of three healthcare professions — alongside physicians and nurse practitioners — qualified to provide primary care. EMS was not mentioned. PAs achieved licensure recognition in all fifty states by 2016.
The results are measurable. The PA profession has been rated among the top careers in America by multiple national rankings — repeatedly, across multiple years. Median PA compensation exceeds that of paramedics by a factor of roughly three. The profession does not have a recruitment crisis, but it has a surplus of qualified applicants.
And the PA profession accomplished all of this without a Federal Office of Physician Assistants. There is no such office. There is no Federal Office of Nursing, either. The two largest non-physician healthcare professions in the United States built national coherence, credentialing standardization, educational infrastructure, and political influence without a dedicated federal agency to coordinate their efforts. They built it from the profession outward.
EMS, by contrast, has spent decades calling for a lead federal agency — a single office in Washington with the authority and resources to coordinate what the profession has not coordinated for itself. That call is not inherently misguided. EMS did have federal architecture, and it was taken away. The grievance is legitimate. But the demand for a federal office in 2026, when every comparable profession has demonstrated that professional coherence can be built without one, raises a question the profession has not confronted directly: is the call for a federal EMS office a policy solution, or is it a substitute for the internal professional development work that PAs, nurses, and pharmacists did on their own?
In each case, the professions that climbed did so by choosing discomfort over stagnation. They accepted short-term workforce disruption as the price of long-term professional viability. EMS, confronted with the same choice, has so far chosen stagnation—and framed the choice as wisdom.
The question is why. Not why any single decision was made — each can be rationalized in isolation — but why the pattern persists across decades, across issues, across every opportunity for structural advancement. That pattern has a name, and a historical precedent older than the profession itself.
The medieval guild is one of history’s most instructive institutions, and one of its most misunderstood. Guilds were not villains. They were rational organizations of skilled workers who banded together to protect wages, regulate competition, control entry into their trades, and ensure quality standards. A stonemason’s guild in fourteenth-century Florence established collective bargaining, apprenticeship standards, mutual aid for members and their families. The guild system worked, often brilliantly, for the guild’s members.
A necessary and important clarification. My guild parallel is not a critique of organized labor. Unions that fight for fair compensation, safe working conditions, sustainable scheduling, and professional recognition are not engaged in guild behavior. They are doing precisely what EMS needs more of — building the structural conditions that allow a workforce to function as professionals rather than subsidize a broken system with their own poverty. The guild parallel describes something different: institutional protectionism that restricts entry, blocks portability, resists accountability, and defends fragmentation — regardless of whether the actor is a union, a credentialing body, a state agency, or an individual provider. The distinction matters because the structural reforms this book calls for will not succeed without organized labor. Public funding, compensation reform, and national standards are all union objectives. The question is whether the institutions of EMS will pursue them, or whether they will default to protecting the architecture they inherited. That is the line between the guild and the union. One defends the current structure. The other fights to build a better one.
The problem was what the guild system did to everyone else.
Over time, guild protections calcified into barriers. Entry requirements were designed less to ensure competence than to restrict competition. Innovation was discouraged because new methods threatened existing practitioners’ market position. Knowledge was hoarded rather than disseminated. The apprenticeship model, originally a mechanism for quality assurance, became a mechanism for artificial scarcity. And because guild members genuinely believed they were protecting the integrity of their craft—and in many cases they were, at least initially—the transition from quality protection to market protection happened so gradually that the distinction dissolved.
The monasteries of the same era exhibited a parallel pattern. They preserved manuscripts, and this was an invaluable contribution to the survival of ancient knowledge. But they also controlled access to those manuscripts, restricting literacy and learning to a narrow institutional class. The monks were not malicious. They believed they were safeguarding sacred knowledge from corruption. The net effect, however, was a centuries-long suppression of the very knowledge they claimed to protect. The manuscripts survived. The civilization that might have used them was delayed.
These historical parallels are directly relevant to the current state of American EMS. In multiple, documented instances, institutional actors within the profession are pursuing strategies that mirror guild-era protectionism: restricting portability, resisting educational advancement, diluting national standards, opposing accountability mechanisms, and blocking clinical innovation. Doing this while framing these positions as protection of the workforce, of patient safety, or of local control. The positions are understandable from a hyper-local perspective, or perhaps from a theoretical labor-protection standpoint. The question is whether they serve the profession’s long-term interests or perpetuate its marginalization.
Chapter 8 — The Enemy Within
The broken promise of 1981 explains the resistance. The guild mentality perpetuates it. But explanations are not exonerations, and at some point the question shifts from why does the profession resist reform to what is that resistance costing it. The examples that follow answer the second question. They are documented, recent, and in most cases still unfolding.
In May 2024, Michigan Governor Gretchen Whitmer signed Senate Bill 249, creating a state-specific paramedic certification examination as an alternative to the National Registry of EMTs examination.40 The bill’s stated purpose was to address Michigan’s paramedic shortage. Its actual mechanism was to create a lower-barrier pathway to paramedic certification that would be, by design, non-transferable to other states. The bill’s own legislative analysis was candid on this point: the state-specific exam was intended, in part, to “keep paramedics in the State.”40
Read that rationale carefully. The solution to a workforce shortage was not to improve compensation, working conditions, or career advancement pathways. The state chose not to address the core factors that research consistently identifies as drivers of recruitment and retention. Conversely, the ‘solution’ was to create a credential that failed to adhere to national standards, would be easier to obtain, and would make it harder for Michigan paramedics to leave. This is not a workforce development strategy. It is a mobility restriction dressed in the language of workforce development. Critics noted at the time that the real solutions—higher wages, better benefits, sustainable scheduling, and professional recognition—were precisely the reforms that would have required investment rather than merely legislation.40
The real solutions required investment. The legislature chose legislation.
As documented in Chapter 7, several states have maintained alternative examinations for decades — inherited fragmentation the profession has been slowly resolving. Michigan's action is categorically different: the deliberate creation of new fragmentation in 2024, reversing decades of progress toward national unity.
The net effect is not more paramedics. It is a fragmented credentialing landscape in which the meaning of “paramedic” varies by jurisdiction—precisely the condition that the national certification system was designed to prevent.
A necessary clarification. The argument here is not against state sovereignty. States possess clear constitutional authority to license medical professionals, and that authority is not in dispute. If Michigan, or any state, wishes to create a state-specific provider level with its own scope of practice, training standards, and credential, that is a legitimate exercise of regulatory power. My objection is narrower and more precise: do not call it a paramedic.
However, the professional title Paramedic carries a specific meaning: it was purposefully created, it is a nationally recognized credential with defined educational standards, requires a validated certification examination, and a scope of practice that the public, the medical community, and the federal reimbursement system all understand. When a state creates an alternative pathway that does not meet those standards and attaches the same title, it does two things simultaneously. It dilutes the credential for every paramedic in every other state, and it misleads the public about what they are receiving when a "paramedic" arrives on their ambulance. If the provider level is genuinely different, and by design, it is, then honesty demands a different name. A state-specific credential that cannot transfer to another state, does not meet the national certification standard, and was explicitly designed to be easier to obtain is not a paramedic by any definition the rest of the profession recognizes. Call it what it is. Let the public make informed decisions about the care they are receiving.
The reimbursement question follows directly. Medicare reimburses at the ALS level because that level carries a defined set of clinical capabilities validated by a standard. A state-created alternative that does not meet that standard should not, in this author's view, be eligible for the same federal reimbursement. To allow otherwise is to use federal dollars to subsidize a credential that was designed to circumvent the standard those dollars were meant to support. States have every right to create their own provider levels. They should not have the right to bill the federal government as though those levels are something they are not.
But perhaps the most telling dimension of the Michigan episode is what did not happen. The profession, nationally, was largely silent. There was no large coordinated outcry from paramedic organizations in other states, no national campaign to defend the integrity of the credential, no collective response remotely proportional to what the legislation represented. Colleagues in other states treated it as a local matter: it's not my state, so it's not impacting me.
Consider the counterfactual. If Michigan had created a non-nurse alternative to a registered nurse (a state-specific "RN" that did not require passing the NCLEX and could not transfer to other states but still titled “RN”) the American Nurses Association, state nursing boards, and nursing educators nationwide would have mobilized within days. Likewise, if a state had created a non-physician alternative to an MD or DO, the response from organized medicine would have been immediate, unified, and overwhelming. These professions understand that a credential is only as strong as its universal meaning, and that an attack on that meaning in one state is an attack on the profession everywhere. EMS did not respond that way. The silence was itself a diagnosis. The painful evidence of a profession that has not yet developed a unified identity or the institutional cohesion to defend its own standards, even when those standards are being explicitly undermined.
In 2025, the Florida legislature passed House Bill 975, a comprehensive healthcare accountability measure requiring fingerprint-based background screening for all licensed healthcare practitioners in the state.41 The legislation's scope was sweeping: dentists, psychologists, nurses, pharmacists, physical therapists, massage therapists, clinical social workers, respiratory therapists were all brought under the unified fingerprint-based criminal history records screening requirement for medical professions. The logic was straightforward: healthcare practitioners who touch patients should be subject to robust background verification.
Tragically, EMTs and paramedics were specifically exempted.41
The example is cited here not as an indictment of a single state, but because it illustrates a broader pattern. Across the country, when comprehensive healthcare accountability legislation is drafted, EMS is routinely omitted, sometimes by deliberate advocacy from within the profession, sometimes by legislative oversight, and sometimes because EMS simply was not at the table when the legislation was written. Whether the exclusion in any given state resulted from active resistance, passive neglect, or institutional invisibility, the outcome is the same: EMS ends up outside a standard that every other healthcare discipline meets. The question the profession must ask itself is not just why this keeps happening, but why, in any of these cases, EMS did not demand to be included.
So, effective July 1, 2025, every other licensed medical professional in Florida is held to a higher transparency and public accountability standard than the paramedic who administers medications, performs invasive procedures, and makes life-or-death clinical decisions in the field.
The exemption may have resulted from deliberate advocacy, legislative oversight, or some combination of both — but whatever the mechanism, the outcome speaks for itself. Perhaps some argued that fingerprint screening would impose undue financial burden on an already strained workforce. The argument was not entirely without merit—fingerprint screening does carry a $40–$50 one-time cost and a minor processing delay. But the decision to exempt EMS from a standard applied to every other category of hands-on healthcare practitioner sends a message about how EMS views and positions itself relative to the rest of the healthcare system. And it sends that message to legislators, stakeholders and our medical colleagues at precisely the moment when EMS is arguing for greater clinical recognition, expanded scope of practice, and parity with other healthcare disciplines.
There is a dimension to this exemption that extends beyond professional positioning. The public already assumes this is being done. Parents who call 911 for a seizing child, elderly patients who open their doors to uniformed strangers, vulnerable individuals encountered alone in private homes — they reasonably believe that the paramedic standing in front of them has been vetted to at least the same standard as their child's daycare worker, teacher, nurse or their massage therapist. They would be stunned to learn otherwise. The EMS exemption is not merely a failure of professional self-advocacy, but it is a breach of implied public trust — one the public does not yet know has occurred.
EMS cannot simultaneously claim clinical equivalence and regulatory exemption. The two positions are logically incompatible. Yet segments of the profession attempted exactly that, and they succeeded.
You cannot simultaneously claim clinical equivalence and regulatory exemption.
Florida's exemption is not an outlier. The 2020 National EMS Assessment, produced by the National Association of State EMS Officials with NHTSA funding, documented that the standard for criminal background checks of EMS professionals varied so widely across states that some relied entirely on self-declaration (the applicant simply affirming no criminal history) while others conducted no background check at all.60 In December 2023, the Interstate Commission for EMS Personnel Practice issued a formal position paper declaring what state EMS directors already knew: "Reliance on self-disclosure for criminal background is both ineffective and unreliable." The Commission urged every state and territory to adopt mandatory FBI-compliant biometric criminal history screening for EMS licensure, calling the action "crucial for public health and safety."61
The EMS Compact requires all member states to implement FBI-compliant criminal history record information checks as a condition of membership in the interstate compact. As of early 2026, twenty-five states have joined the Compact, and for those states, fingerprint-based background screening is a legal obligation written into each state's legislation. That represents genuine structural progress in building a national framework that makes background screening a prerequisite rather than a preference. The Commission's own 2023 position paper was addressed not to its members, but to "every state and territory across the United States," an acknowledgment that the problem the Compact was built to solve has not yet been solved nationally.
The pattern is consistent. The profession has not lacked for frameworks, recommendations, or institutional urgency on accountability. What it has lacked is the collective will to make a single standard universal, and to insist that EMS be included, rather than exempted, when the rest of healthcare raises the bar.
In 2018, a coalition of organizations issued a joint position statement opposing any mandatory degree requirement for paramedic certification.42 The statement argued that “no identifiable data” supported the claim that formal education improves patient outcomes and warned that mandatory degree requirements would trigger a workforce collapse by erecting barriers to entry in an already understaffed profession.
The same year, a coalition of EMS educators and medical directors published a counterargument. Caffrey et al. (2018) argued that the associate degree should be established as the minimum educational standard for paramedic certification, noting that virtually every other allied health profession—nursing, respiratory therapy, physical therapy, occupational therapy—had already adopted or was in the process of adopting degree mandates as a condition of professional recognition.43 The educator coalition did not claim that degrees were a panacea. They argued that degree requirements were a necessary structural foundation for professional legitimacy; the same argument that every other healthcare discipline had already accepted and acted upon.
The educator coalition was not operating in isolation. Two years earlier, the National EMS Advisory Council — the federal advisory body to NHTSA — had formally recommended that the Department of Transportation convene a multidisciplinary task force to develop formal paramedic degree programs at the associate, baccalaureate, and graduate levels, concluding that "EMS providers are educated and certified outside of the formal education industry" and are therefore "often not perceived as health care providers, have limited ability to influence the overall health care system, and are reimbursed at a lower rate."59 As of 2026, that recommendation remains unimplemented.
The irony of the degree debate is sharpened by a historical fact that the profession has largely forgotten. The EMT-Paramedic (as it was titled in 1975) was not created external to the allied health system. It was created inside it. The paramedic profession was created following the identical pathway that every other allied health profession used to establish itself.
In 1966, Congress passed the Allied Health Professions Training Act, which granted the American Medical Association nationwide authority to approve allied health professions and accredit the institutions authorized to educate them. By the early 1970s, the AMA's Committee on Allied Health Education and Accreditation — CAHEA — was accrediting over twenty-three allied health program types at hundreds of institutions. Physician Assistants went through this system. Respiratory therapists went through it. Surgical technologists, perfusionists, radiologic technologists — all of them followed the same structural pathway:
AMA recognition as a bona fide health occupation
establishment of a Joint Review Committee
development of accreditation standards
a national certifying examination administered by an independent board.
In early 1975, Dr. J.D. "Deke" Farrington, as Chair of the Board of the National Registry of EMTs, and Rocco V. Morando, the NREMT's Executive Director, formally petitioned the AMA's Committee on Health Manpower to recognize the "Emergency Medical Technician – Paramedic" as a "bonafide emerging health occupation." The petition was not a vague aspiration. It was a detailed, ten-page submission titled "Guidelines for the Development of a New Health Occupation: EMT – Paramedic," and it included a defined scope of duties, educational standards, background requirements, employment projections, professional certification requirements, and a plan for national recertification. The document specified that training programs would be "conducted in medical and educational institutions having the necessary available clinical facilities" and projected an initial output of 10,000 EMT-Paramedics annually from universities, medical schools, junior colleges, hospitals, and state educational systems. It called for all paramedics to be certified by the National Registry and periodically reexamined. The NREMT's board of directors at the time included physicians, fire and police chiefs, the Ambulance Association of America, the National Ambulance and Medical Services Association, and the National Funeral Directors Association — the full coalition of the era, unified behind a single professional standard.52
The AMA's response, dated February 7, 1975, is equally telling. John J. Naughton, Secretary of the Department of Health Manpower, wrote back that the NREMT had done "a fine job of assembling the data in compliance with our guidelines" and engaged substantively on workforce projections, compensation ranges, and whether paramedics would function solely on ambulances or also within hospital emergency departments, coronary care units, and intensive care units. The AMA was not humoring a fringe request. It was processing a legitimate application from an emerging health profession; through the same institutional machinery it used for every other allied health discipline. In April 1975, the AMA approved the request. A Joint Review Committee on Education Programs for the EMT-Paramedic was established and the accreditation standards (the "Essentials for EMT-Paramedic Program Accreditation") were adopted. By 1978, the first NREMT EMT-Paramedic examination was administered. By 1980, UCLA and Eastern Kentucky University became the first programs to receive formal accreditation.
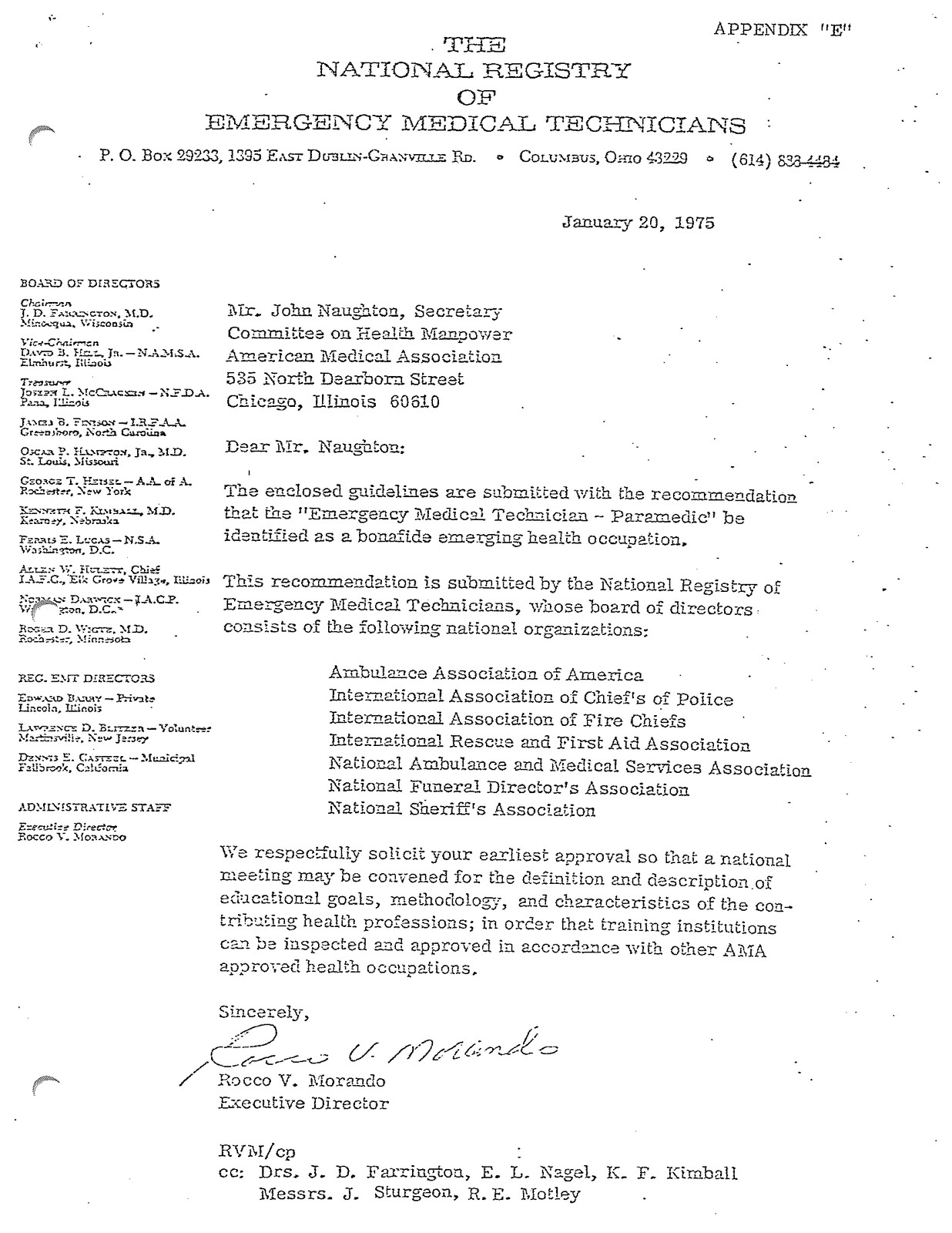
Again, the structure to become an EMT-Paramedic was identical to what the physician assistant profession had built in the early 1970s, and what respiratory therapy and surgical technology had built before that. The paramedic was deliberately created as an allied health professional, recognized by organized medicine, accredited through the same system as every comparable discipline, and validated by a national certifying examination. The physicians who championed this pathway — Farrington, Safar, Caroline, and others — understood that professional legitimacy required institutional architecture, and they built it.
What happened next is the divergence that defines the degree debate. Physician Assistants, who went through the same AMA-CAHEA system at the same time, progressively raised their educational floor: from certificate programs in the 1960s, to bachelor's programs, to master's-level education as the standard by 2000. Today, PA programs require a master's degree for entry, are accredited by an independent commission that evolved from CAHEA, and PAs practice with clinical autonomy, prescriptive authority in all fifty states, and Medicare provider status. Respiratory therapists raised their floor from associate to baccalaureate. Physical therapists moved from bachelor's to master’s, and now a clinical doctorate. In each case, the profession (collectively and internally) used its accreditation infrastructure — the same infrastructure the paramedic was given in 1975 — as the foundation for educational advancement and professional recognition.
EMS diverged and chose to go the other direction. As paramedic programs expanded rapidly in the 1980s and 1990s, many did not seek accreditation. Many were not affiliated with colleges or universities. State EMS offices, still nascent and inconsistent, lacked the regulatory capacity to enforce uniform standards.
The NREMT did not initially require graduation from an accredited program as a condition of eligibility for the national paramedic examination. This was a policy gap that would not be closed until 2013. But the nature of that gap deserves careful attention, because it was not a design flaw. It was a failure of imagination. The NREMT's own board members — physicians and EMS leaders who had personally petitioned the AMA, who had built the Joint Review Committee, who had invested years of professional capital in establishing the EMT-Paramedic as a recognized allied health occupation — had created the national examination as the capstone of a system they assumed the nation would embrace. They had made the sacrifice and the investment to birth a new profession within the established architecture of American healthcare. It would have been nearly inconceivable to them that the beneficiaries of those efforts would so quickly disregard the very foundation their mentors had built. No other health profession had even contemplated such a revolt against standards. Physician Assistant programs, Physical Therapy, Occupational Therapy, Respiratory Therapy programs all used the foundation as the base to develop academic programs. The assumption that paramedic programs would follow the same trajectory was not naïve, but it was based on the universal pattern of every allied health profession that had come before. The NREMT did eventually formalize the requirement through policy, mandating accredited program graduation for paramedic examination eligibility by 2013. But the fact that such a policy was necessary at all — that the profession's own national licensure exam body had to compel what every comparable discipline had adopted voluntarily — tells you everything about where the divergence began.
The allied health infrastructure that the founding physicians had painstakingly constructed was not destroyed by external forces. It was simply viewed as optional. The scaffold was built. The profession chose not to climb it.
That context reframes the entire degree debate. When opponents of educational mandates argue that degree requirements are an external imposition alien to the profession's identity, they are making a historically false claim. The paramedic was an allied health profession. It was recognized as one by the AMA, accredited as one by CAHEA, and built on the same foundation as the physician assistant, the respiratory therapist, and the occupational therapist. The question is not whether EMS should become an allied health profession with degree standards. The question is why it stopped being one.
The consequences of that divergence are not merely historical. On February 5, 2026, the Drug Enforcement Administration published a final rule creating, for the first time, a DEA registration category for EMS agencies. This was implementing a law Congress had passed nine years earlier.57 Until that rule took effect, EMS agencies had no independent federal registration to handle controlled substances. They operated under hospital registrations, either as hospital-owned extensions or through formal agreements to act as a hospital's agent. The DEA's own rulemaking acknowledged that the Controlled Substances Act had never even mentioned EMS prior to the 2017 legislation. Physician assistants, nurse practitioners, pharmacists, and dentists have held independent DEA registrations for decades. The paramedic, who administers Schedule II controlled substances in uncontrolled field environments, without a physician physically present, was the last healthcare practitioner in America to receive independent federal recognition for that authority. The allied health framework for EMS was built in 1975. Fifty-one years later, the federal government was still building the basic regulatory infrastructure that the profession's own divergence had delayed.
When I refer to choices the profession made, I am not referring to you, the paramedic working a seventy-two-hour week, or you the EMT driving ninety minutes to transfer a patient because the nearest hospital closed, or you the volunteer keeping a rural service alive on personal sacrifice alone. I have been all three.
The providers on the front lines did not choose to abandon professionalism, education, or alignment with the established allied health pathway. In most cases, they were never told it existed. The decisions documented here were made gradually over decades by institutional leaders, organizational boards, state regulators, and professional associations who set the structural direction of the profession on behalf of a workforce that was too busy keeping people alive to attend the meetings where its future was being decided. The indictment in this chapter is directed at the institutional level, not the individual one. The providers are not the problem. In many cases, they are the ones paying the highest price for decisions made above them and, in some cases, before them.
With that distinction drawn, the institutional arguments against educational advancement deserve examination on their own terms.
The “no identifiable data” claim deserves scrutiny. It is true that no single randomized controlled trial has demonstrated that a paramedic with an associate degree produces better patient outcomes than a certificate-trained paramedic in a specific clinical encounter. It is also true that no such study is likely to be conducted, because the variables in prehospital care—system design, medical direction, protocol variation, transport time, receiving facility capability—make outcome-level comparisons between individual provider credentials methodologically intractable. But the absence of a specific study is not the absence of evidence. The broader literature on healthcare workforce development consistently demonstrates that higher educational attainment correlates with professional autonomy, expanded scope of practice, higher compensation, greater regulatory recognition, and stronger institutional standing. These are not incidental benefits. They are the structural preconditions for professional advancement. Nursing did not wait for a randomized trial proving that BSN-prepared nurses produce measurably better outcomes in every patient encounter before mandating the baccalaureate. The profession recognized that educational standards are the mechanism through which professions gain standing, and that waiting for a perfect study was a strategy for permanent stagnation.
The practical gap between a certificate and an associate degree in paramedicine is, in most accredited programs, a single semester of additional coursework. Two-thirds of accredited paramedic programs already offer the associate pathway. The debate is not whether to impose a radically different educational model. It is whether to formalize what the majority of quality programs are already doing.
And as with every healthcare profession that has raised its educational floor, current practitioners must be grandfathered forward. The paramedics and EMTs practicing today should not be penalized for meeting the standards that existed when they entered the profession. They should continue to practice, continue to contribute, and play a central role in mentoring the next generation. Raising the bar for new candidates is not an indictment of those who preceded them. It is the natural progression of a maturing profession—the same progression that nursing, respiratory therapy, and physician assistant education all navigated without dismantling their existing workforce.
A 2020 doctoral dissertation by Newton-Riner examined why EMS failed to professionalize along the trajectory of comparable healthcare disciplines.44 Among the findings was a cultural identity conflict within EMS itself: a divide between providers who conceptualize their role in "how" terms and those who conceptualize it in "why" terms. The "how" orientation focused on task execution, protocol compliance, and procedural skill. The "why" orientation focused on clinical reasoning, diagnostic judgment, and pathophysiology.
Newton-Riner argued that the "how" orientation, reinforced by public safety culture and non-degree-based training, actively resists the educational reforms that would shift the profession toward a "why" orientation. The dissertation also identified what it characterized as "oppression by physicians". This was categorized as the persistent subordination of EMS clinical autonomy to physician oversight structures. I disagree with that characterization and believe it deserves qualification considering both the historical record and the legal reality of EMS practice.
Historically, the physicians who built the EMT-Paramedic — Farrington, Safar, Caroline, Nagle, McSwain… — did not subordinate the profession. Rather, they constructed its professional architecture, championed its AMA recognition, and designed the accreditation pathway that every other allied health discipline used to achieve autonomy.
Legally, the characterization misapprehends the nature of EMS licensure itself. In nearly all states, EMTs and paramedics do not practice under a physician's license. They are individually licensed as medical professionals, independently accountable under the provisions of their own license. If there is a complaint or if a paramedic commits a clinical error, it is the paramedic that is held accountable. Assuming the medical director properly screened the paramedic, verified that training and education were current, and established medically appropriate protocols, the medical director generally bears no individual liability for the paramedic's clinical decisions in the field. In most states, it is not delegated practice; EMTs and Paramedics are not practicing under the physician’s license. It is independent licensure with medical oversight. This is an important distinction that matters enormously: EMS providers already possess, in law, a degree of professional autonomy that the "oppression" framing fails to recognize.
What later generations of EMS providers may experience as physician control is, in significant part, the natural consequence of a profession that has not completed the educational and credentialing progression its founders designed for it. A physician assistant who holds a master's degree and practices under a collaborative agreement does not experience that relationship as oppression. An EMS provider who is, in legal fact, already individually licensed may feel constrained by medical direction. But the remedy was always available, and it was the same remedy every comparable profession adopted: raise the educational floor, and the professional recognition follows.
The conflict Newton-Riner identified is a consequence of the divergent path of EMS: a profession that was created in an allied health framework (parallel to Physician Assistants) and walked away from it, and now experiences the predictable constraints of that decision as external oppression rather than internal consequence.
There is another structural artifact of the profession's first-aid origins that quietly constrains its advancement, one so deeply embedded that most EMS professionals have never questioned it: the state-credentialed EMS instructor.
In most states, an individual cannot teach an EMT or paramedic course without holding a state-issued instructor certification or license endorsement. Although the specific requirements vary by state, the model is broadly consistent: the prospective instructor must hold an EMS credential at or above the level being taught, complete an instructor training course, and receive approval from the state EMS office.
I will share a personal experience that illustrates how deeply embedded this model is — and how invisible it becomes to those inside it.
When I arrived in Colorado as the new State EMS Director, one of my first priorities was transferring my professional credentials. I completed the paramedic license application without difficulty. Then I went looking for the EMS Instructor application. I searched the state website. I checked every form, every link, every dropdown menu. Nothing.
When I asked the previous director where to find the instructor application, she paused, smiled slightly, and said, "You may want to sit down."
Colorado did not have state-certified EMS instructors.
I was at a loss for words. I had held an EMS Instructor certification for over twenty-five years. I had earned it, maintained it, transferred it between multiple states. It was not just a credential — it was a symbol of work, pride, accomplishment, and professional standing. And I had just walked into a state that had simply... decided not to issue one.
Before I could voice my frustration, she continued: "Before you react, look at the data. Our National Registry pass rates are consistently among the best in the country."
Then came the question that I have never been able to shake: "Have you ever considered why state EMS offices are the only medical profession that issues individual instructor certifications? It's just not how the other professions work."
She was right. On both counts.
That conversation reframed my understanding of a structure I had spent a quarter century accepting without question. Colorado had not abandoned a standard — it had simply never adopted an assumption that the rest of healthcare had never shared in the first place.
Here’s the irony, subject matter experts who are not state-certified EMS instructors are usually restricted to teaching a limited percentage of the course, if they are permitted to teach at all. A cardiac surgeon with a medical doctorate and decades of clinical experience may not be authorized to teach cardiology in a paramedic program unless that physician also holds a state EMS instructor certification, or a state-certified paramedic instructor is in the classroom “supervising”. Likewise, in many states, an individual with a PhD in pathophysiology would be prohibited from teaching the subject they have spent a career mastering. Or, they may be permitted to deliver only a small fraction of instructional hours under the supervision of a certified instructor whose own educational credentials may be substantially less advanced.
Now pause and consider this: When was the last time you encountered a state-certified physician instructor? A state-certified nursing instructor? A state-certified dentist instructor, occupational therapist instructor, physical therapist instructor, or pharmacist instructor?
Have you ever stopped to ask this question?
The concept is so foreign to every other healthcare profession that it sounds like a joke. It does not exist. In nursing, physician assistant education, respiratory therapy, pharmacy, and every other professional discipline, instructor qualifications are determined by the accredited educational institution, not by a state regulatory agency certifying individuals to teach. The institution is responsible for hiring qualified faculty, and the accrediting body holds the institution accountable for the quality of its educational program. The state's role is to ensure that the institution meets accreditation standards, not to individually approve every person who stands in front of a classroom.
So, why is EMS different?
Consider where does this concept of individual instructor certification exist?
First aid & CPR. Courses where a national organization, the American Heart Association or the American Red Cross, certifies individuals to deliver their educational content in a standardized, scripted format, with their specific curriculum, in community settings.
That is the origin of the EMS instructor model.
Remember the 1960s. The federal government gave money to states to increase the number of people certified in basic first aid. That was the initial basis of the rebuilding of EMS. The people closest to the problem, those already teaching first aid, were upgraded to teach the new EMT National Standard Curriculum (NSC). In fact, the NSC-EMT was itself engineered as a standardized, heavily scripted curriculum delivered in community settings. This was structurally identical to the first-aid and CPR courses it evolved from.
A network of state-certified instructors was created to deliver that program. However, the paramedic pathway was purposefully created differently. As documented in the preceding section, the founders designed paramedic education within the allied health system — college-based, accredited, and structurally identical to physician assistant and respiratory therapy programs, none of which use state-level individual instructor certification. But when that framework fragmented in the 1980s, the distinction collapsed. As local efforts scrambled to sustain paramedic training outside the institutional structures the founders had built, the state-certified instructor model — designed for standardized community first-aid courses — expanded to fill the vacuum. The EMT instructor model became the paramedic instructor model by default, not by design.
The state-certified instructor model is not merely a historical curiosity. It has practical consequences. State EMS offices are among the most underfunded regulatory offices in state government. The resources those offices allocate to individually approving, tracking, renewing, and auditing instructor certifications are resources that are not being directed toward institutional oversight, program accreditation support, quality improvement, or system development. The last thing a state EMS office should be doing, in my personal opinion, is individually approving people to teach. That is not a productive use of limited state resources. The state should be evaluating whether institutions are delivering proper education. If they are not, the state should hold the institution accountable. Let the institution determine who is qualified to deliver instruction within its programs. If a program can recruit a physician with a PhD in pathophysiology to teach pathophysiology, that should be a win for everyone, not a regulatory violation.
This is not an argument against instructor education. I believe individuals teaching in any discipline should invest in learning how to teach effectively. Pedagogy matters. Instructional design matters. The ability to translate clinical knowledge into effective learning experiences is a skill that deserves deliberate development. Excellent instructor development courses and certification programs exist—the National Association of EMS Educators' instructor course among them—and these should be actively pursued as markers of external competency and professional commitment. But that development should be a professional expectation managed at the institutional level, not a state regulatory function that consumes limited resources and produces a bottleneck that restricts who can contribute to EMS education.
The pattern is the same one that runs through every section of this chapter. A structure that made sense in the profession's infancy, when EMS was closer to a community first-aid program than a licensed medical profession, has been carried forward into an era where it no longer serves the profession's interests. The state-certified instructor model is an invisible anchor, one that most EMS professionals accept without question because it has always been there. But "it has always been there" is not a justification. It is a symptom of a profession that has not yet examined which of its inherited structures are foundations and which are fossils.
If we want to progress as a medical profession, we have to structure our education like a medical profession. That means accredited institutions, accountable for outcomes, empowered to hire the best available faculty. It means state resources focused on the areas of highest return: institutional quality, not individual instructor approval. It means trusting the same accreditation model that every comparable healthcare discipline has already adopted and proven. The model already exists. The question is whether the profession will adopt it.
Perhaps, one of the greatest mistakes in retrospect was the decision to model EMT education after Community First Aid training. The enduring impact of the First Aid certified drivers and ambulance attendants of the 1950s & 1960s is not limited to the current educational design of EMS, but also the core terminology.
The terminology itself reveals the problem's depth. When states began tracking EMS providers, they were tracking the number of people certified in first aid. Certification, in that context, meant demonstration of a specific competency, a designation that could be conferred and tracked. When the EMT was created, it represented something fundamentally different. States were not merely certifying a competency. They were granting permission to practice a medical profession, an authority that derives from the police powers clause of the United States Constitution. That is a license. It does not matter what the state calls it. Some states to this day refer to EMTs and paramedics as "state certified" rather than "state licensed," a terminological holdover from the first-aid era that carries real consequences.
Too often, I hear our own professional colleagues assert that because they are "not licensed" by the state, they have a lower standing than other legitimate licensed professions. I have also heard false arguments from licensed colleagues in other disciplines incorrectly assert that a state-certified paramedic is lesser because they are not "licensed." The terminology used by the state, while incorrect and confusing, does not change the legal reality: it is a state-granted permission to practice a medical profession, restricted by state authority and enforceable by law. If you doubt this, let your state certification lapse and continue to practice. You will learn about the police power authority of a state to regulate and limit professional practice very quickly.
Interstate licensure portability is not a new concept. In 2026, nearly twenty healthcare professions operate interstate compacts — physicians, nurses, physical therapists, psychologists, audiologists, counselors — allowing qualified practitioners to work across state lines without obtaining separate licenses in each state. These compacts are authorized by the U.S. Constitution, upheld by the Supreme Court, and operational in every state. The framework is settled law, not experimental policy.
The EMS Compact follows the same structural logic. Developed in 2013–2014 by a coalition that included state EMS officials and representatives of both labor and management organizations — funded by the Department of Homeland Security, which identified a national security need for mobile EMS personnel. The EMS Compact removes the administrative burden of duplicate state licenses, but it does not change scope of practice, medical director authority, agency regulations, or any other aspect of how EMS is practiced within a state. A paramedic using the Compact must still affiliate with a local agency, practice under local medical direction, and follow local protocols. Twenty-five states have enacted it with a ninety-eight percent legislative approval rate. The Department of Defense designates occupational licensure compacts as the "gold standard" for professional licensure portability.45
Federal law reinforces this designation. The Servicemembers Civil Relief Act (SCRA), which protects military spouses and service members from the burden of re-licensure when relocated across state lines, explicitly defers to occupational licensure compacts where they exist. When an EMS Compact state receives a military-affiliated provider, the Compact's own provisions supersede the federal statute's protections — because Congress recognized that compacts already provide the portability framework the SCRA was designed to approximate.
Despite this, several state-level EMS stakeholder organizations have opposed the EMS Compact and similar portability initiatives. The arguments converge on familiar concerns: portable credentials will undercut local wages, employers will import cheaper labor, and "local control" requires local credentialing authority.45
Each argument dissolves under examination. The wage concern assumes that restricting provider supply is the solution to low compensation. This strategy (unique and non-standardized state specific licensure requirements) has been in effect for decades without producing the promised wage gains. The cheap-labor argument's own logic is revealing: if the concern is that out-of-state providers will accept lower wages, the implication is that current wages are already insufficient — which is precisely the problem the Compact's opponents claim to be addressing through other means.
The concern about EMS compensation is not only legitimate — it is one of the most urgent issues facing the profession. The question is whether restricting interstate mobility is an effective mechanism for addressing it, and the evidence of the past several decades suggests it is not.
The "local control" argument, examined closely, often functions as a proxy for institutional protectionism: preserving jurisdictional authority over credentialing not because it improves patient care, but because it preserves the institutional power of the credentialing body.
There is also a patient safety consequence to portability opposition that its proponents rarely acknowledge. Today, individuals whose EMS licenses are revoked or restricted in one state for public-protection reasons can seek licensure in non-Compact states, where no reliable mechanism exists — absent self-disclosure — to identify prior disciplinary action or criminal convictions. The Compact closes that gap through mandatory reporting of adverse actions within two business days and a coordinated database that provides real-time visibility across all member states. Opposition to the Compact is not merely opposition to workforce mobility. It is, in effect, opposition to the only operational mechanism that prevents bad actors from exploiting regulatory blind spots between states. The irony is sharp: the same organizations that frame their opposition as protecting patient safety are resisting the framework that most effectively provides it.
The guild parallel is precise. Medieval guilds restricted the mobility of skilled workers to protect local markets. The same dynamic operates when state-level organizations resist a portability framework that every other major healthcare profession has already adopted. The opposition does not come from patients, medical directors, state legislatures, or the federal government. The opposition, again, is originating from within the profession itself, and the cost of that opposition is no longer merely philosophical. Non-Compact states are increasingly disadvantaged in federal funding programs — the Rural Health Transformation grant, for example, awarded points to Compact states and penalized non-Compact states — meaning that internal resistance to portability is now directly reducing the federal resources available to the communities these organizations claim to protect.
The preceding examples involve legislative and policy battles where institutional positions can be traced through public records. But the resistance to advancement extends beyond formal policy into the operational culture of the profession itself.
The 2024 EMS Trend Report by Fitch & Associates, an annual survey of EMS agencies nationwide, has documented a persistent pattern of innovation resistance that is difficult to attribute to external barriers alone.46 Across consecutive survey years, the data shows: sixty-five to seventy-one percent of agencies have not adopted telemedicine capabilities; approximately seventy-five percent have not implemented protocols for arranging alternative transportation for patients who do not require emergency department transport; sixty-six percent have not adopted transport to alternative destinations such as urgent care or mental health facilities; and ninety percent do not equip field providers with body-worn cameras.46
These are not experimental technologies or untested concepts. Telemedicine is operational in virtually every other healthcare delivery setting. Alternative transportation and alternative destination protocols have been demonstrated in pilot programs and adopted by progressive agencies for years. Body-worn cameras are standard in law enforcement—a field that EMS frequently cites as a professional peer. The failure rates documented in the Trend Report are not failures to adopt bleeding-edge innovation. They are failures to adopt practices that are routine in adjacent professions and have been available, in many cases, for over a decade.
The ET3 (Emergency Triage, Treat, and Transport) pilot program offers a case study in how innovation resistance and structural inertia compound each other. ET3 was a Medicare initiative designed to test payment models that would reimburse EMS agencies for treating patients in place or transporting them to alternative destinations—precisely the kind of clinical flexibility that EMS leaders have publicly advocated for years.
The results were devastating. CMS selected 205 applicants for ET3, but only 185 executed participation agreements. Of those 185, fewer than half—just 70 agencies—ever delivered a single paid ET3 intervention. Nationally, across three full years of operation from 2021 through 2023, the entire program produced 3,397 interventions, including just 253 transports to alternative destinations. Eight higher-volume agencies accounted for nearly three-quarters of all interventions; the remaining 62 active participants averaged roughly fifteen patients each across the entire three-year model.
The medical triage line component was cancelled outright when CMS received only 29 applications for up to 40 cooperative agreements. There were not enough EMS agencies participating to support evaluation. CMS terminated the model two years early, ending it on December 31, 2023, after concluding that intervention volumes were far below projections and inadequate to justify continued operation or a robust evaluation.47
Multiple factors contributed, and intellectual honesty requires acknowledging that some were legitimate. The COVID-19 pandemic struck during ET3’s first two performance years, diverting agencies to crisis operations. CMS prohibited participants from marketing TIP and TAD to patients in advance, meaning people in medical distress were hearing about these alternatives for the first time during an emergency—patient refusal rates ran from forty to over eighty percent among even the highest-volume participants. Obtaining agreements with alternative destination partners was the primary implementation challenge, cited by half of all respondents to CMS learning system surveys. Technology connectivity problems, particularly in rural areas, limited telehealth delivery. These were real obstacles, and agencies that chose not to participate were not uniformly choosing complacency.
But the barriers themselves are evidence. A profession that had been operating as healthcare providers rather than transporters would have had relationships with urgent care facilities, mental health centers, and primary care offices already in place. A profession with clinical infrastructure would not have needed to build telehealth capability from scratch in the middle of a pandemic. A profession whose crews routinely exercised clinical judgment beyond the transport decision would not have experienced what CMS documented as “disengagement among EMS ambulance personnel”—resistance so pervasive that the only agencies achieving meaningful volume were those that required crews to offer ET3 options as standard protocol and invested in ongoing monitoring of compliance. The structural barriers to ET3 were not bad luck layered on top of a functional system. They were the architecture of the transportation model—the very architecture this book has documented—expressing itself when asked to perform as something it was never built to be.
The numbers, even accounting for every legitimate obstacle, tell a story that transcends logistics. The federal government offered EMS precisely what the profession said it wanted: payment for treating patients in place, payment for transport to alternative destinations, clinical flexibility beyond the transport-only model. The profession’s collective response, nationwide, was 70 agencies and 3,397 interventions in three years. When the door to the cathedral was opened, most of the profession did not walk through it.
The internal resistance documented above does not occur in a vacuum. It occurs in the context of a profession that is, by international standards, already an outlier.
O’Meara49 conducted a comparative analysis of EMS professionalization across high-income countries and concluded that the United States is exceptional; but not in the way its practitioners might hope.49 American EMS is characterized by lower educational requirements, greater fragmentation of credentialing, weaker professional autonomy, and a cultural identity more closely aligned with public safety than with healthcare. O’Meara observed that American paramedics “often self-identify as public safety providers” rather than as healthcare professionals. This is an identity orientation that is both a product and a perpetuator of the profession’s structural marginalization.49
In Australia, the United Kingdom, and much of the European Union, paramedics hold bachelor’s or master’s-level degrees, practice with significant clinical autonomy, and are integrated into national healthcare systems with dedicated funding streams. The contrast is not minor. It is categorical, and the internal resistance to educational advancement, credentialing standardization, and clinical innovation documented in this chapter is the mechanism by which the gap persists.
The professions that successfully raised their educational floors—pharmacy, nursing, and respiratory therapy—are examined in Chapter 7. The pattern is consistent: each accepted short-term disruption as the price of long-term professional viability. EMS, confronted with the same choice, has so far chosen stagnation—and framed the choice as wisdom.
There is also a dimension of individual harm that is rarely discussed. Certificate-trained paramedics who later pursue higher education often discover that their paramedic training, which may have taken eighteen months or longer, carries little or no transferable college credit. They must effectively start over. The current system does not merely fail to advance the profession. It actively disadvantages the individual providers it claims to protect.
The monks who hoarded manuscripts believed they were protecting knowledge. The guilds that restricted entry believed they were protecting quality. In both cases, the belief was sincere, and in both cases, the net effect was the opposite of the stated intention. Knowledge that is protected from circulation ceases to function as knowledge. Quality that is defined by exclusion rather than excellence ceases to function as quality. Protection, taken past its rational limit, becomes suppression.
The institutional actors within EMS who oppose portable credentials, resist educational advancement, dilute national standards, exempt the profession from accountability frameworks, and block clinical innovation are not, in most cases, acting from malice. They are acting from a rational calculation of institutional self-interest: protect the current workforce, protect local authority, protect existing operational models, protect the jobs and wages of current members. These are legitimate concerns, and they deserve acknowledgment.
There is also a deeper dynamic at work, one that deserves naming even if it does not alter the conclusion. Decades of chronic underfunding, political neglect, broken reimbursement, and cultural dismissal have produced a profession that has, in measurable ways, internalized the low expectations imposed on it from outside. When a workforce is told for long enough that nothing will change, it stops investing energy in change and redirects that energy toward endurance. Scarcity becomes not a condition to be overcome but an identity to be defended. Broken systems are protected not because they work but because they feel like the only systems available. Reformers are treated as threats rather than allies, because reform implies that the adaptations people built their careers around were insufficient — and that implication is personal in a way that policy language rarely captures. This psychology is real, it is understandable, and it explains a great deal of what this chapter documents. But it does not excuse it. Nursing internalized similar messages for decades before choosing to reject them. Respiratory therapy operated under the same structural constraints before deciding those constraints were unacceptable. Every profession that climbed out of institutional neglect had to first recognize that the ceiling it had accepted was not a ceiling at all but a choice it had stopped questioning. The psychology of adaptation explains why the guild defends the wall. It does not obligate the profession to keep doing so.
But acknowledgment is not endorsement. The question is not whether these positions are understandable. The question is whether they serve the profession’s long-term survival or accelerate its marginalization. And the evidence assembled in this chapter points overwhelmingly in one direction.
A profession that creates non-portable credentials to prevent its own practitioners from leaving the state is not building a workforce. It is building a wall.
A profession that exempts itself from background screening standards applied to all other medical professionals is not protecting its members. It is advertising its unseriousness.
A profession that opposes degree requirements adopted by every comparable healthcare discipline is not defending access. It is defending the status quo.
A profession in which seventy-five percent of agencies have not adopted alternative transport protocols—while simultaneously arguing that it deserves clinical recognition—is not resisting change. It is resisting itself.
The pattern across every example in this chapter is the same contradiction: demanding professional recognition while rejecting professional standards. Demanding clinical parity while seeking regulatory exemption. Demanding workforce investment while opposing workforce mobility. Demanding respect while resisting accountability. These positions are not merely inconsistent. They are irreconcilable. Legislators and the rest of the healthcare system see the contradiction clearly, even if segments of our own profession do not.
The pattern is not theoretical. It is being documented in real time, by the profession's own institutions and by state legislatures across the country.
In 2018, the Idaho Legislature commissioned town hall meetings to address the collapse of volunteer EMS. The findings were sobering: volunteers had dropped from sixty-four percent of Idaho's EMS workforce in 2002 to forty-one percent by 2018, and the total EMS workforce had barely grown despite significant population increases.53 The cost to replace those volunteers with paid personnel was estimated at $72.9 million per year—a figure unchanged from a similar assessment six years earlier, indicating not just a crisis but a frozen one. The recommendations that emerged were strikingly modest: employer recognition programs, broadband internet access for rural fire stations, thirty-thousand-dollar pilot programs for community paramedicine. These were not the recommendations of a profession planning its future. They were the recommendations of a profession managing its decline.
The federal advisory council itself had reached the same conclusion years earlier. NEMSAC formally recommended in 2012 that "EMS should be considered an essential service" and that "appropriate steps must be taken by all stakeholder communities to ensure continued sustainable funding mechanisms for EMS Systems". This recommendation was reaffirmed in 2016 and 2019, and it remains unimplemented.58
In 2021, NAEMT issued a position statement that should have been unnecessary. It argued that EMS should be recognized as an essential public function—a designation that fire and law enforcement have held for generations. The statement acknowledged what the profession already knew:
"Both the Fire Service and Law Enforcement are funded through governmental sources; EMS relies on a fragmented and inadequate patchwork of financing despite its essential public function."54
A 2016 federal survey found that ninety-two percent of the American public already believed EMS was an essential service, and seventy-seven percent believed communities should fund it the way they fund police and fire. The public was not the obstacle. The institutional architecture was.
In December 2022, Maine's Blue Ribbon Commission delivered its findings to the state legislature. Every transporting EMS service in Maine was operating at a loss. Medicare reimbursement covered roughly $492 per call regardless of whether the actual cost was $710 or $2,522. The commission identified what it called the largest subsidy underwriting EMS in the state: "volunteer and underpaid labor." It found a $70 million annual funding shortfall and concluded that EMS was "at the edge of a cliff" or, in many rural areas, already over it. The authorizing legislation itself had to formally establish that EMS provided by an ambulance service constitutes an essential service—meaning that in 2022, the state of Maine had not yet legally recognized what ninety-two percent of the public already assumed.
In September 2025, Colorado's EMS System Sustainability Task Force delivered its Phase III report to the General Assembly. Twenty percent of the state's EMS clinicians planned to leave within twelve months.56 Among those aged twenty to twenty-nine, more certified clinicians were not practicing than were. Seventy percent of EMS calls in Colorado did not involve transport—and received no reimbursement whatsoever. The report documented that seventy-five percent of fire-based EMS personnel earned over $81,000 annually, while seventy-five percent of non-fire EMS workers performing the same clinical work earned under $80,000. The disparity was not a function of skill, training, or patient outcomes. It was a function of organizational structure, not clinical competence.
The compensation disparity is not an argument against fire-based EMS. It is an argument against a system that makes a paramedic’s economic standing dependent on which patch they wear rather than what clinical care they deliver. Two paramedics with identical training, identical certifications, performing identical clinical interventions on identical patients should not earn fundamentally different wages because one is employed by a fire department and the other by a private ambulance service or a county third-service agency. The disparity does not prove that fire-based EMS is overpaid. It proves that everyone else is underpaid—and that the mechanism by which fire-based EMS achieves adequate compensation (public funding) is the same mechanism this book argues should be extended to the entire profession.
Multiple states, spanning seven years, producing independent reports that arrive at the same conclusions. Volunteer systems collapsing. Reimbursement models that pay for transport but not for care. A workforce hemorrhaging at every level. Two-tier compensation for identical clinical work depending on organizational structure. And still, in 2021, the profession's largest national association found it necessary to formally argue that EMS should be recognized as an essential public function — a designation that fire and law enforcement have held for generations. That the argument still had to be made is itself the indictment — not of the association that made it, but of a system that had failed to act on what should have been self-evident decades earlier. And in every report, the recommendations stop short of the structural transformation the data demands — not because the authors lacked insight, but because the institutional frameworks within which they operated constrained the range of solutions available to them. You cannot recommend dismantling a funding model from inside the system that model sustains.
These reports are not discovering new problems. They are rediscovering the same ones, because the profession has not yet diagnosed the underlying disease. The symptoms are contemporary. The pathology is historical.
The Dark Ages of EMS, as documented in the preceding chapters, were imposed from the outside. The wars, the Depression, the funeral industry’s capture of ambulance services, the federal government’s failure to build sustainable funding—these were forces that the profession could not control. But in 2026, significant portions of the contemporary resistance to EMS advancement seem to be originating from within the profession’s own institutional structures. The enemy is no longer exclusively external.
If EMS remains in a prolonged dark age—marginal, underfunded, under-credentialed, and clinically constrained—it will not be because the external barriers were insurmountable. It will be because the profession’s own institutional actors chose protection over progress, certainty over discomfort, and the guild over the cathedral.
But honesty requires an additional acknowledgment. The resistance documented in this chapter is not purely a failure of will. Much of it is a rational response to a broken incentive structure—a structure the profession did not design and does not control. People who resist educational mandates they cannot afford on EMS wages are not irrational. They are trapped. Understanding why they are trapped, and what it would take to free them, requires one more chapter.
The monasteries eventually opened their libraries. The guilds eventually gave way to professional licensing. The question for American EMS in 2026 is whether it will lead that transition or be overtaken by it. History suggests that professions which refuse to reform themselves are eventually reformed by forces far less sympathetic to their members’ interests than the reformers they resisted. The railroad did not choose to become irrelevant. It chose not to change—and irrelevance was the consequence.
The door to the cathedral is open. The only question is whether the guild will walk through it.
History suggests that professions which refuse to reform themselves are eventually reformed by forces far less sympathetic to their members' interests.
Chapter 9 — Knowing Where We Came From
The argument of this book is simple, even if its implications are not. America built sophisticated emergency medical systems before the world wars destroyed them. The nation rebuilt, brilliantly but incompletely, on compromises it intended to replace. It never did.
Everything else—the funding crisis, the credentialing fragmentation, the workforce collapse, the professional marginalization—flows from that unfinished work. The floor that was supposed to be temporary became the ceiling. The financial architecture of the Dark Ages transport-only model was encoded into Medicare and never reformed. And the profession itself, shaped by a broken federal promise and decades of institutional neglect, internalized constraints that it now defends as identity.
But what distinguishes the EMS Dark Ages from the medieval ones is that we need not wait centuries for a renaissance. The knowledge exists. The clinical capability exists. The workforce exists. The technology exists. What does not yet exist—in many states, in many communities, and at the federal level—is the political and financial architecture to support what everyone already knows is essential.
The evidence is everywhere. Between 2018 and 2025, state legislatures from Idaho to Maine to Colorado independently commissioned studies of their EMS systems and arrived at the same conclusions this book reaches through historical analysis: the financial model is broken, the workforce is unsustainable, and the structural architecture inherited from the rebuilding era was never designed to support what EMS has become. Maine's Blue Ribbon Commission found that the single largest subsidy keeping EMS operational was volunteer and underpaid labor—and that even with that subsidy, every transporting service in the state was operating at a loss. Colorado documented that up to seventy percent of EMS responses generate no reimbursement at all because they do not result in transport. Idaho calculated that replacing its collapsing volunteer workforce with paid professionals would cost $72.9 million annually. These are not historical artifacts. They are dispatches from the present—independent analyses, conducted years apart in different states, arriving at the same conclusions because the underlying pathology is the same. I championed the law that established Colorado's EMS System Sustainability Taskforce and co-wrote Colorado's year-one report. I know the people who wrote the others.
The diagnosis is not in dispute. The question is why the treatment keeps being deferred. This book offers part of the answer — not the policy prescription, but the historical framework without which no prescription can be complete.
I did not write it to produce a policy agenda. Others are doing that work, and some of them are doing it well. I wrote it because I believe the EMS profession cannot build what it needs to build if it does not understand the history and what it has already lost—and why we lost it. The paramedics and EMTs who staff this fractured system deserve to know that the problems they face every shift are not evidence of a young profession still finding its way. They are the inherited consequences of a collapse that happened nearly a century ago, a rebuilding that was never completed, and an institutional culture that has, in too many cases, made peace with the result.
I have not made peace with it.
I have spent a career inside this profession—as a volunteer paramedic in communities where I was the only advanced provider, as an instructor and program director, as a state EMS director, and now working at the national level to build the interstate infrastructure that the 1981 collapse should never have made necessary. I have seen what EMS looks like when the architecture is built right. I helped design and build national EMS systems in foreign countries, including Sri Lanka. It is a country with a fraction of America's resources, but their EMS system was recently regarded by the World Bank as "one of the world's most digitally advanced" ambulance services, noted for its "remarkable efficiency and setting new standards for government-delivered services."62 The people and the government of Sri Lanka decided that emergency medical services were essential, and then the nation ensured the system was funded. It was not easy. It was not fast. But it was not impossible, and the fact that it happened at all is proof that the barriers American EMS faces are not immovable. They are choices. And choices can be unmade.
The physicians who built this profession—Farrington, Safar, Caroline, and the others documented in these pages—did not make peace with inadequacy. They saw a system that had failed and they built something extraordinary inside the established architecture of American healthcare, with the full institutional backing of organized medicine. They gave the profession a scaffold. They assumed the profession would climb it. They were building for the generation that came after them, and the generation after that.
We are those generations. The question that faces us is not whether we honor their work with gratitude. It is whether we honor it with action.
Senator Reed said, "We're not ready to designate emergency medical services as essential—yet."
That single word—yet—carries the weight of this entire book. It acknowledges both the present failure and the possibility of change. It is an honest word, a legislator's word, measured and conditional. And it is the word that EMS has been living inside for seventy years.
The question is not whether EMS has come a long way. It has. The question is whether we will finish what the rebuilders of the 1960s started, or continue to mistake the temporary for the permanent, the floor for the ceiling, and the compromise for the plan.
The historical argument of this book is now complete. But its application is not. The final chapter examines what this history means for the profession right now—how the structural decisions documented in these pages manifest in the specific funding crises, workforce debates, and reform efforts of 2026 and beyond. The history is not offered as an ending. It is offered as a lens, and what that lens reveals about the present may be the most important argument this book makes.
That single word — yet — carries the weight of decades of struggle and consequence.
Chapter 10 — The Sixty-Year Illusion
In 2026, the emergency medical services profession is celebrating its sixtieth anniversary. The milestone is being marked in trade journals, at conferences, and across the institutions that were built in the decade following the 1966 White Paper. It is a natural occasion for reflection, and the story being told is a good one: from nothing, in a single lifetime, a profession was created that now responds to tens of millions of emergencies every year across the United States. The story is true, but it is also the most consequential illusion in American emergency medicine.
American ambulance based out of hospital medical care is not sixty years old. It is more than a hundred and sixty years old. What the profession is celebrating in 2026 is not its birth. It is the sixtieth anniversary of its reconstruction—the second time the nation built organized emergency medical systems, not the first. The first-time produced physician-staffed, hospital-integrated, publicly funded ambulance services in American cities before the twentieth century began. The Great Depression hollowed them out. Two world wars stripped them of personnel. The funeral industry filled the vacuum with hearses. And by the time the White Paper authors surveyed the wreckage in 1966, the earlier systems had been so thoroughly forgotten that the report read as a discovery of something new rather than a recognition of something lost.
The preceding nine chapters have documented this full arc in detail. This chapter is not a summary of that history. It is the payoff. Because the illusion of a sixty-year-old profession is not merely a historical error. It is a structural one, and it produces structural consequences. A profession that believes it started from nothing in 1966 accepts its current crises as the growing pains of a young field still finding its way. A profession that knows its actual history recognizes those crises for what they are: the inherited consequences of a collapse that happened nearly a century ago and a reconstruction that was never completed. The first diagnosis produces patience. The second produces urgency. And patience, at this point, is something American EMS can no longer afford.
The sixtieth anniversary is a milestone. It marks the most extraordinary rebuild of a public service in American history. It is also a measure of how long the reconstruction has remained unfinished.
The call for a lead federal EMS agency deserves more honest examination than it typically receives. Before the profession asks for a new federal home, it should acknowledge the one it has.
The Department of Transportation, through NHTSA’s Office of EMS, has been the most consistent and dedicated long-term federal partner this profession has ever had. NHTSA funded the development of the original EMT curriculum. It built and maintains the National EMS Information System—the most comprehensive prehospital data infrastructure in the world. It provides technical assistance to state EMS offices, funds evidence-based guideline development, supports state EMS system assessments, and administers grant programs that reach every state in the nation. When no other federal agency would sustain a commitment to emergency medical services, NHTSA did. That commitment continues today, and it would be both historically inaccurate and strategically reckless to frame it as a problem to be solved.
The problem is not that EMS has a home at the Department of Transportation. The problem is that EMS has a home only at the Department of Transportation.
The clinical dimension of the profession—reimbursement, provider classification, workforce development, integration into the healthcare data ecosystem—has no comparable federal architecture on the healthcare side. NHTSA cannot reclassify ambulance services from suppliers to providers within Medicare. That authority belongs to the Centers for Medicare and Medicaid Services. NHTSA cannot include paramedic education in the Title VII healthcare workforce funding that supports nursing and physician assistant programs. That authority belongs to the Health Resources and Services Administration. NHTSA cannot write EMS into the interoperability standards that govern health information exchange. That authority belongs to the Office of the National Coordinator for Health Information Technology. The clinical work that EMS performs every day is governed by federal agencies that have no institutional relationship with the profession—and the federal agency that does have that relationship was never designed to address clinical policy.
What EMS needs at the federal level is not a choice between transportation and healthcare. It needs both. It needs NHTSA’s Office of EMS to continue and expand what it already does—the technical assistance, the data infrastructure, the education standards, the highway safety mission that remains a core part of what EMS responds to every day. And it needs a complementary architecture on the healthcare side that addresses the clinical identity the profession has been building for sixty years: provider classification that reflects clinical reality, reimbursement that pays for care rather than transport alone, workforce development funding that treats paramedic education the way federal programs already treat nursing and physician assistant education, and data integration that connects the prehospital record to the healthcare systems it serves.
The profession routinely calls for a federal EMS office, but it has not yet defined with precision what that office would do. A funding coordination center? A regulatory home within the healthcare framework? A technical assistance hub modeled on the National Fire Academy? A seat at healthcare policy tables where EMS is currently absent? These are different things, and they require different institutional solutions. The physician assistant profession and the nursing profession built national coherence without a dedicated federal office. But neither profession had to overcome a federal classification that actively denied its clinical identity. EMS must do both: build professional coherence from within, and correct the federal architecture that works against it from without. Those are not competing strategies. They are complementary ones.
The reconstruction this book has documented left EMS with half an architecture. NHTSA built and sustained one side. The other side—the healthcare side—was never constructed. Finishing the reconstruction means building what is missing, not dismantling what works.
The problem is not that EMS has a home at DOT. The problem is that EMS has a home only at DOT. Finishing the reconstruction means building what is missing, not dismantling what works.
Every one of these reform conversations gains explanatory power from the history documented in this book. That is not because the history provides all the answers. It does not. It is because the history explains why the questions keep recurring. The same crises, rediscovered every decade, documented by new commissions, addressed with new pilots, and never resolved—because the foundation on which all of these efforts rest was compromised from the beginning. You can refinish a floor that has settled. You can repaint walls that have cracked. At some point, you have to address the foundation, or the repairs become permanent.
The practitioners and policy leaders doing this work are not wrong. They are working with the best information available to them, and they are producing real results within the constraints they inherited. What this book offers is additional information—the historical context that transforms the reform conversation from how do we fix this to why does this keep breaking. The first question produces operational solutions. The second produces structural ones. Both are needed. But the profession has been disproportionately invested in the first, and the results speak for themselves: fifty years of operational solutions that leave the structural conditions unchanged.
Chapters 7 and 8 of this book documented a pattern of internal resistance to professional advancement: opposition to portable credentials, resistance to educational standards, exemption from accountability frameworks, institutional defense of the compromised architecture. I stand behind every word of that documentation. The pattern is real, it is costly, and it must be named.
But naming a pattern is not the same as understanding it. And the history this book has uncovered makes one thing unmistakably clear: the resistance, in most of its forms, is rational. It is counterproductive, but it is rational. And understanding why it is rational is the prerequisite to changing it, because you cannot change behavior by demanding that people act against their own interests. You change behavior by changing the interests.
Start with the degree debate, because it is the one that generates the most heat and the least light. The argument against educational mandates in EMS almost always begins with economics: paramedics cannot afford degrees on paramedic wages. That argument is correct. Median paramedic compensation in the United States makes a degree requirement functionally punitive for a working provider who is already subsidizing the system with below-market labor. The response from education advocates—that degrees will eventually raise compensation, as they did in pharmacy, nursing, and the PA profession—is also correct, historically. But it asks the current generation of providers to absorb a cost whose benefits will accrue to the next generation. That is a difficult argument in any profession. It is an impossible argument in a profession where the average provider is already volunteering the gap between what the system costs and what the system pays.
The burden falls hardest on rural and volunteer systems, where the barrier is not only cost but access. Degree programs may not exist within a hundred miles. The communities these providers serve cannot offer compensation competitive with urban systems regardless of educational requirements. A national educational standard imposed without addressing the geographic and economic realities of rural EMS does not elevate the profession. It abandons the communities that need it most.
Here is what the historical context reveals. Paramedic wages are low because EMS is funded through a billing model that reimburses for transport, not for clinical care—a model that was imposed during the reconstruction, not chosen by the profession, and documented in Chapter 6 of this book. The degree resistance and the funding crisis are not separate problems. They are the same problem, expressed at different points in the same structural chain. Fix the funding architecture, and the degree debate resolves itself, because adequately compensated professionals can afford professional education and the education pays for itself in career advancement. Attempt the degree mandate without fixing the funding, and you produce exactly the resistance documented in Chapter 8—not because the resisters are opposed to education, but because they are being asked to invest in a credential the system will not reward.
But the structural diagnosis does not justify the structural delay. No healthcare profession in American history waited for compensation reform before raising its educational standards — not pharmacy, not nursing, not the Physician Assistant profession. In every case, the profession raised its education first, endured a difficult transition, and watched compensation follow as the credential gained market value and regulatory standing. The argument that EMS should be the exception — that providers should be paid more before being asked to learn more — is not only historically unprecedented, it inverts the mechanism by which every comparable profession achieved the compensation its practitioners deserved. Education is the lever. It has always been the lever. The funding architecture must be fixed, and this book has made that case at length. But waiting for the fix before advancing education is not pragmatism. It is the same pattern this book has documented across 160 years: accepting an incomplete reconstruction as permanent because finishing the work is hard.
The tension is real but not irreconcilable. The resistance is understandable at the individual level. It is difficult for a working paramedic on minimum wage to absorb the cost of an associate degree, knowing that even upon completion, their salary will not change. The resistance is historically unjustified at the institutional level—the organizations that set the profession’s structural direction have the capacity to advocate for both reforms simultaneously, and their failure to do so is a choice, not a constraint. The degree debate is not a choice between education and compensation. It is a failure to demand both at the same time, the way every comparable profession does. The individual provider’s calculus is rational. The institutional leadership’s acceptance of that calculus as permanent is the problem this chapter documents.
The same structural logic applies across every front of the resistance. Agencies resist tiered response not because they are philosophically opposed to smarter deployment, but because they fear liability in a reimbursement system that still measures value by transport volume and response time. The ET3 pilot offered clinical flexibility, and seventy-two agencies participated nationwide across three years46—not because the rest of the profession rejected the concept, but because agencies looked at a time-limited pilot in a system that had already abandoned the national EMS infrastructure once before and made a rational calculation about institutional risk. Unions resist scope changes because they have watched the profession promise elevation before and deliver nothing.
The fire-EMS relationship illustrates the structural diagnosis precisely. Fire departments stepped into EMS in community after community because they had what independent EMS agencies lacked: a tax-funded infrastructure with political standing, union protection, and institutional permanence. In many of those communities, fire-based EMS is the strongest, most sustainable model available — and it works, in large part, because fire departments brought EMS under a public funding umbrella that the profession never had on its own. Colorado’s 2025 report documented the result: seventy-five percent of fire-based EMS personnel earned over eighty-one thousand dollars while seventy-five percent of non-fire EMS workers performing identical clinical work earned under eighty thousand.56 That disparity is not evidence of fire service overreach. It is evidence that public funding works where it exists — and that EMS providers outside the fire service are paying the price for a funding model that was never extended to them. The question is not whether EMS belongs in fire departments. For many communities, it does, and it works. The question is why the financial architecture that makes fire-based EMS sustainable has never been built for the profession as a whole.
The international evidence confirms the structural diagnosis. In nations where EMS is funded as a public good—the United Kingdom, Germany, Japan, the systems documented in Chapter 6—the resistance patterns that dominate American EMS discourse largely do not exist. There is no degree debate in the UK or Australia, because paramedic education is funded as part of the healthcare workforce pipeline, and graduates enter a profession that compensates them accordingly. There is no portability crisis in nations with national licensure frameworks. There is no fire-EMS cultural divide in systems where every EMS provider — regardless of organizational model — operates under the same funding framework and professional standards. The resistance is not a feature of emergency medical services. It is a feature of American emergency medical services—specifically, of the structural conditions that the American reconstruction created. Change the conditions, and the resistance dissolves, because the rational calculus that produces it no longer applies.
This reframing matters because it changes the nature of the conversation the profession needs to have with itself. The resistance documented in Chapter 8 is real and costly. But it will not be overcome by stronger arguments, better data, or more compelling conference presentations. It will be overcome by changing the structural conditions that make resistance the rational choice. When the funding model rewards clinical care instead of transport volume, agencies will adopt clinical flexibility without requiring a federal pilot to test the concept. When compensation reflects professional education, providers will pursue degrees without mandates to compel them. When the credentialing system is nationally coherent, portability will be the default rather than the exception. The reform sequence matters: fix the structure first, and the behavior follows.
The people inside the resistance are not the enemy. The structure they inherited is the problem. But they perpetuate the structure when they resist the changes that would fix it—and at some point, the distinction between defending your own interests within a broken system and defending the broken system itself becomes a distinction without a difference.
You are not the problem. The structure you inherited is the problem. But you perpetuate the structure when you resist the changes that would fix it.
This book is a history, not a policy blueprint. Others are writing those blueprints, and some of them are writing them well. But the history documented in these pages does not merely explain the past. It identifies the structural conditions that must change if the profession is going to stop cycling through the same crises every decade. Those conditions are not mysterious. They are not controversial. And in most cases, they are already being met somewhere in the world.
Fund EMS as a public good. The argument is made in detail in Chapter 6, and it does not require restating here. What requires stating is that this is not a theoretical position. Police and fire have operated under collective public funding for as long as both services have existed in the United States. The question is not whether public funding for emergency services works. The question is why one of the three legs of the emergency response triad was rebuilt under a different model—and the answer, as this book has documented, is historical accident, not policy design. Fire-based EMS systems already operate under this principle, and their relative stability demonstrates that the model works. The argument is not that fire departments should stop providing EMS. It is that every EMS provider — regardless of organizational structure — deserves the same financial foundation that makes fire-based EMS sustainable.
The organizational model — what the profession increasingly distinguishes as the service delivery model — matters less than the system within which it operates. Fire-based, third-service, hospital-based, private, volunteer — each can deliver excellent emergency medical care when the system's funding architecture, clinical standards, and professional framework support it. Private ambulance operators deserve particular recognition in this context: they have built and sustained EMS in communities across the country, often on margins so thin that a single policy change or payer shift can threaten viability. Unlike municipally operated services that can draw on a local tax base as a financial backstop, private operators absorb disproportionate uncompensated care costs with no public safety net beneath them. That they have sustained operations at all under these conditions is a testament to operational discipline — and an indictment of a system that forces any provider, public or private, to treat insolvency as a business model. The goal is not to dictate where EMS is housed. It is to ensure that regardless of service delivery model, the system is funded as a public good, integrated into healthcare, and held to a single national professional standard.
Build the healthcare-side federal architecture that was never constructed. As documented earlier in this chapter, the problem is not EMS's partnership with DOT — it is the absence of a complementary partnership on the healthcare side. The clinical consequences of that absence are documented in Chapter 6: transport-only reimbursement, supplier rather than provider classification, exclusion from health information exchange, separation from the healthcare workforce development programs that fund every other clinical profession. These are not DOT failures. They are HHS gaps. Closing them requires building institutional relationships between EMS and the federal healthcare agencies — CMS, HRSA, the Office of the National Coordinator — that govern the clinical dimensions of what the profession does every day. The reconstruction left half the architecture unbuilt. This is the half that remains.
Finish building national licensure portability. The EMS Compact demonstrates that the profession can build national coherence from within — without a federal mandate, without waiting for Washington, through the same kind of state-by-state institutional work that the PA and nursing professions used to build their own infrastructure. But the Compact is not yet law in all fifty states. And if this book has demonstrated anything, it is that half-built solutions in EMS have a way of becoming permanent.
The 1973 EMS Systems Act was half-built — its regional system design held enormous potential, but when federal funding collapsed, implementation fragmented. That single failure explains why some states today have robust regional systems with dedicated funding and coordinated oversight, while others have no regional infrastructure at all. The credentialing system followed a different path but the same pattern: the NREMT was created by the most powerful medical body on the planet — the AMA — with direct support from the White House and President Johnson. It was designed as a national standard from the beginning. But as federal commitment evaporated and states fragmented, the NREMT was left to sustain that vision alone. It took forty years of patient rebuilding before forty-eight states finally realigned around national credentialing — a reconstruction still not complete. The funding model remains half-built. In every case, the urgency that started the work dissipated before the work was finished.
The EMS Compact cannot become another example of that pattern. The Emergency Management Assistance Compact — EMAC — is law in all fifty states because the nation recognized that disaster response cannot stop at state lines. The same logic applies to emergency medical services. A paramedic's credential should not expire at a border any more than a hurricane does. The EMS Compact must be passed in every state, and the profession must treat anything less than universal adoption as unfinished work — not as progress to be celebrated but as a reconstruction still underway.
Link education requirements to compensation reform. The degree debate, as currently framed, is a false choice. Raising educational standards without addressing the funding model that produces poverty wages is punitive. Raising wages without raising standards produces a better-paid but still marginalized workforce. The two reforms are interdependent, and every profession that successfully raised its educational floor—pharmacy, nursing, respiratory therapy, physician assistants—did so in conjunction with structural changes that made higher education economically viable for the workforce and professionally rewarding for graduates. EMS cannot be the exception to that pattern and expect a different result.
The structural reforms described in this chapter — public funding, compensation tied to professional education, national standards — are not achievable without organized labor. They are, in fact, union objectives by another name.
Integrate EMS into the healthcare system it serves. Chapter 6 documented the invisible patient record—the fact that EMS generates clinical data that largely vanishes at the emergency department door. That invisibility is not a technology problem. It is an identity problem, and it flows directly from the same structural conditions that produced the funding crisis. A system classified as transportation does not need to share clinical records, because a transportation system does not generate clinical care. But EMS generates clinical care every day, in every community, and until its information systems, its regulatory frameworks, and its institutional relationships reflect that reality, the profession’s claim to clinical parity will remain unsupported by the most basic infrastructure that every other medical discipline takes for granted. Clinical integration means EMS data flows into the healthcare record. It means EMS outcomes are measured alongside hospital outcomes. It means the paramedic’s clinical judgment is built upon, not repeated, when the patient arrives at the emergency department.
None of this is utopian. I have seen what EMS looks like when the architecture is built correctly. I helped design and build a national EMS system in Sri Lanka—a country with a fraction of America’s resources, where a parliamentary-funded ambulance service now covers twenty-two million people with standardized training, centralized dispatch, and universal coverage.62 The United Kingdom, Germany, Japan, Ireland, and dozens of other nations fund emergency medical services through their national healthcare architectures.
And here is the historical fact that should stay with every reader of this book. The model those nations operate—publicly funded, nationally standardized, clinically integrated emergency medical services—is closer to what American cities built in the 1880s than to what America has today. The physician-staffed ambulances of New York, Chicago, and Cincinnati were funded by municipal budgets, integrated into hospital systems, dispatched through public communications infrastructure, and staffed by the most qualified medical professionals available. We are not asking for something unprecedented. We are asking for something the nation once had, lost during the Dark Age, and has spent sixty years failing to fully rebuild. The reconstruction that began in 1966 is not finished. This is what finishing it looks like.
I have spent this book making an argument that requires the reader to accept something uncomfortable: that the structural problems of American EMS are not developmental. They are inherited. They were not caused by the people working in the system today, but they are sustained by a system that those people have the power to change—if they choose to, and if they understand what they are changing and why.
The argument carries an implication that is both difficult and necessary. If the problems are structural, then better leadership alone cannot solve them. A better chief, a better state director, a better national organization—none of these can overcome a funding model that was designed to fail, a federal classification that denies the profession’s clinical identity, or a credentialing system fragmented by a forty-five-year-old federal betrayal. Individual excellence matters. It is not enough. Structural problems require structural solutions, and structural solutions require a profession that understands its own structural history well enough to demand the right changes rather than the familiar ones.
That is what this book was written to produce. Not a policy agenda. Not an indictment. A historically informed profession. The paramedics and EMTs who answer the call every day deserve to know that the challenges they face every shift are not evidence of their profession’s youth or their own inadequacy. They are the evidence of decisions made decades before most of them were born, by people who intended the compromises to be temporary, in circumstances that made those compromises rational at the time. The compromises were not the failure. Treating them as permanent was the failure. And that failure is within our power to correct.
The sixtieth anniversary of the 1966 reconstruction is the right moment to stop telling ourselves only the reassuring version of our own history. Not because that version is false—the accomplishments since 1966 are real, extraordinary, and built by people who deserve lasting honor. But because the incomplete version produces incomplete solutions. And incomplete solutions, applied for sixty years, are how a profession ends up where American EMS is today: essential in function, marginal in standing, and running out of time to close the gap.
The question is not whether EMS has come a long way. It has. The question is whether the profession will finish what the rebuilders of the 1960s started—or whether it will celebrate another anniversary, commission another sustainability report, document another workforce crisis, and continue to mistake the temporary for the permanent, the floor for the ceiling, and the compromise for the plan.
The history documented in this book is not a sentence. It is a diagnosis. And we are the generation that finally has the knowledge, the evidence, and the professional maturity to write the treatment plan. Now, it’s time to finish the work.
The history is not a sentence. It is a diagnosis. And we are the generation that can finally write the treatment plan.
Dedication
I dedicate this book …
To the advocates championing essential service designation, funding reform, and sustainability legislation — the ones trying to finish what was started.
To the state EMS directors and officials holding a fragmented system together while the work continues.
To the men and women on the ambulances, subsidizing a public service with their labor and their poverty, who deserve better than the architecture they inherited.
And to the National Collegiate EMS Foundation, which for over thirty years has invested in the next generation — the college and university students who answer emergency calls while earning the degrees this profession has been slow to require.
The profession needs its reformers, its stewards, its workforce, and those who invest in its future. This book is for all of them.
Companion Website
For links to many of the reference documents cited in this book, visit the Interactive Timeline and Document Library — the companion digital archive to all of Donnie Woodyard's books on EMS history.
Explore the Timeline →Disclaimer & Legal Notice
The views expressed in this book are solely those of the author and do not necessarily reflect the views of any employer or organization that the author is affiliated with or may have previously been affiliated with. This book represents the author's personal opinions and should not be construed as official statements or positions of any employer or organization.
Every attempt has been made to verify and present factually accurate information, and complete citations to prior works have been provided. However, the author and publisher assume no responsibility for errors or omissions in the citations or the content of the book.
Publication Information
Library of Congress Control Number: 2026903760
ISBN: 979-8-9885254-9-3 (paperback)
LCSH Subjects: Emergency medical services — United States — History. Emergency medical technicians — United States — History. Paramedics — United States — History. Ambulance service — United States — History.
Classification: LCC RA645.5 .W66 2026 | DDC 362.18/80973—dc23
Copyright © 2026 by Donnie Woodyard, Jr. All rights reserved.